

Right vs. left ventricular longitudinal strain for mortality prediction after transcatheter aortic valve implantation
- PMID: 37745112
- PMCID: PMC10513390
- DOI: 10.3389/fcvm.2023.1252872
Right vs. left ventricular longitudinal strain for mortality prediction after transcatheter aortic valve implantation
Abstract
Introduction: This study aims at exploring biventricular remodelling and its implications for outcome in a representative patient cohort with severe aortic stenosis (AS) undergoing transcatheter aortic valve implantation (TAVI).
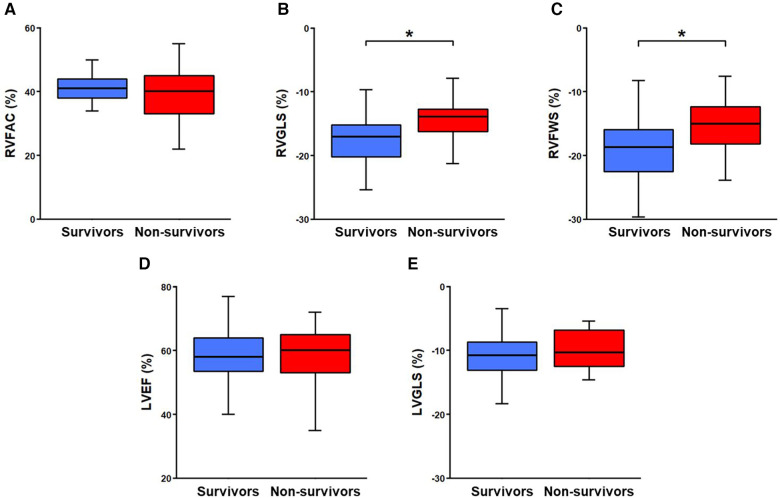
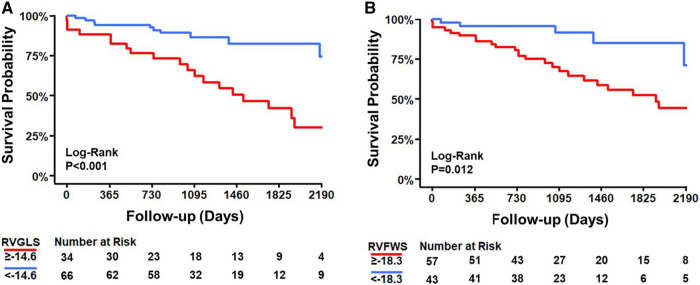
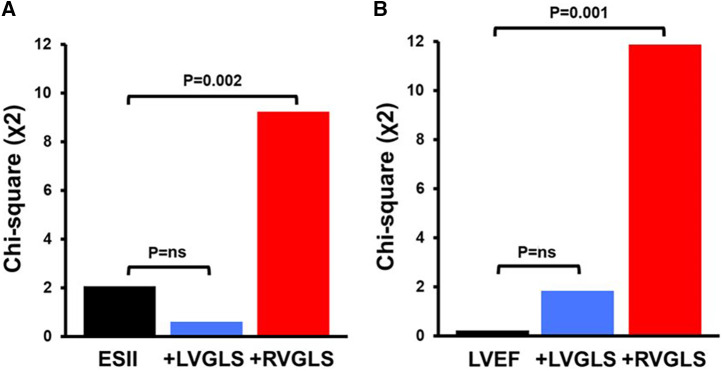
Methods and results: Pre-interventional echocardiographic examinations of 100 patients with severe AS undergoing TAVI were assessed by speckle tracking echocardiography of both ventricles. Association with mortality was determined for right ventricular global longitudinal strain (RVGLS), RV free wall strain (RVFWS) and left ventricular global longitudinal strain (LVGLS). During a median follow-up of 1,367 [959-2,123] days, 33 patients (33%) died. RVGLS was lower in non-survivors [-13.9% (-16.4 to -12.9)] than survivors [-17.1% (-20.2 to -15.2); P = 0.001]. In contrast, LVGLS as well as the conventional parameters LV ejection fraction (LVEF) and RV fractional area change (RVFAC) did not differ (P = ns). Kaplan-Meier analyses indicated a reduced survival probability when RVGLS was below the -14.6% cutpoint (P < 0.001). Lower RVGLS was associated with higher mortality [HR 1.13 (95% CI 1.04-1.23); P = 0.003] independent of LVGLS, LVEF, RVFAC, and EuroSCORE II. Addition of RVGLS clearly improved the fitness of bivariable and multivariable models including LVGLS, LVEF, RVFAC, and EuroSCORE II with potential incremental value for mortality prediction. In contrast, LVGLS, LVEF, and RVFAC were not associated with mortality.
Discussion: In patients with severe AS undergoing TAVI, RVGLS but not LVGLS was reduced in non-survivors compared to survivors, differentiated non-survivors from survivors, was independently associated with mortality, and exhibited potential incremental value for outcome prediction. RVGLS appears to be more suitable than LVGLS for risk stratification in AS and timely valve replacement.
Keywords: aortic stenosis; global longitudinal strain; mortality; speckle tracking echocardiography; transcatheter aortic valve implantation.
© 2023 Winkler, Anwer, Reeve, Michel, Kasel and Tanner.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Incremental Value of Biventricular Strain in Patients with Severe Aortic Stenosis.J Cardiovasc Dev Dis. 2024 Mar 13;11(3):90. doi: 10.3390/jcdd11030090. J Cardiovasc Dev Dis. 2024. PMID: 38535113 Free PMC article.
-
Incremental Prognostic Value of Left Ventricular Global Longitudinal Strain in Patients with Preserved Ejection Fraction Undergoing Transcatheter Aortic Valve Implantation.J Am Soc Echocardiogr. 2022 Sep;35(9):947-955.e7. doi: 10.1016/j.echo.2022.04.013. Epub 2022 Apr 30. J Am Soc Echocardiogr. 2022. PMID: 35504527
-
Change and impact of left ventricular global longitudinal strain during transcatheter aortic valve implantation.World J Clin Cases. 2022 Feb 26;10(6):1806-1814. doi: 10.12998/wjcc.v10.i6.1806. World J Clin Cases. 2022. PMID: 35317147 Free PMC article.
-
Distribution and Prognostic Significance of Left Ventricular Global Longitudinal Strain in Asymptomatic Significant Aortic Stenosis: An Individual Participant Data Meta-Analysis.JACC Cardiovasc Imaging. 2019 Jan;12(1):84-92. doi: 10.1016/j.jcmg.2018.11.005. JACC Cardiovasc Imaging. 2019. PMID: 30621997
-
Prognostic Value of Left Ventricular Global Longitudinal Strain for Major Adverse Cardiovascular Events in Patients with Aortic Valve Disease: A Meta-Analysis.Cardiology. 2024;149(3):277-285. doi: 10.1159/000536331. Epub 2024 Feb 1. Cardiology. 2024. PMID: 38301616
Cited by
-
Impact of Stress Echocardiography on Aortic Valve Stenosis Management.J Clin Med. 2024 Jun 14;13(12):3495. doi: 10.3390/jcm13123495. J Clin Med. 2024. PMID: 38930024 Free PMC article. Review.
-
Preoperative right ventricular strain as an early predictor of perioperative cardiac failure in patients undergoing mitral surgery: An exploratory study.Health Sci Rep. 2024 Jul 23;7(7):e2172. doi: 10.1002/hsr2.2172. eCollection 2024 Jul. Health Sci Rep. 2024. PMID: 39050905 Free PMC article.
-
Pre-interventional renal artery calcification and survival after transcatheter aortic valve implantation.Int J Cardiovasc Imaging. 2025 Jan;41(1):113-122. doi: 10.1007/s10554-024-03295-5. Epub 2024 Dec 7. Int J Cardiovasc Imaging. 2025. PMID: 39644387 Free PMC article.
-
Incremental Value of Biventricular Strain in Patients with Severe Aortic Stenosis.J Cardiovasc Dev Dis. 2024 Mar 13;11(3):90. doi: 10.3390/jcdd11030090. J Cardiovasc Dev Dis. 2024. PMID: 38535113 Free PMC article.
References
-
- Ancona R PCS. Epidemiology of aortic valve stenosis (AS) and of aortic valve incompetence (AI): is the prevalence of AS/AI similar in different parts of the world? (2020); Volume 18. Available at: https://www.escardio.org/Journals/E-Journal-of-Cardiology-Practice/Volum...
-
- Alec Vahanian FB, Praz F, Milojevic M, Baldus S, Bauersachs J, Capodanno D, et al. ESC/EACTS scientific document group. 2021 ESC/EACTS guidelines for the management of valvular heart disease: developed by the task force for the management of valvular heart disease of the European society of cardiology (ESC) and the European association for cardio-thoracic surgery (EACTS). Eur Heart J. (2022) 43(7):561–632. 10.1093/eurheartj/ehab395 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous