

The dichotomy of glucocorticosteroid treatment in immune-inflammatory rheumatic diseases: an evidence-based perspective and insights from clinical practice
- PMID: 37745141
- PMCID: PMC10515127
- DOI: 10.5114/reum/170845
The dichotomy of glucocorticosteroid treatment in immune-inflammatory rheumatic diseases: an evidence-based perspective and insights from clinical practice
Abstract
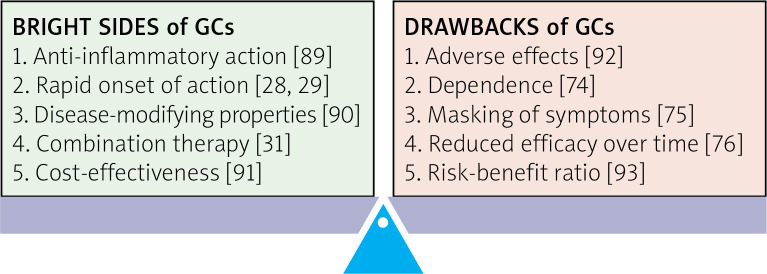
Objectives: Glucocorticosteroids (GCs) are the most used anti-inflammatory and immunosuppressive drugs due to their effectiveness in managing pain and disease modification in many immune-inflammatory rheumatic diseases (IRDs). However, their use is limited because of adverse effects (AEs).
Material and methods: The authors analyzed recent studies, including randomized controlled trials (RCTs), observational, translational studies and systematic reviews, providing an in-depth viewpoint on the benefits and drawbacks of GC use in rheumatology.
Results: Glucocorticosteroids are essential in managing life-threatening autoimmune diseases and a cornerstone in many IRDs given their swift onset of action, necessary in flares. Several RCTs and meta-analyses have demonstrated that when administered over a long time and on a low-dose basis, GC can slow the radiographic progression in early rheumatoid arthritis (RA) patients by at least 50%, satisfying the conventional definition of a disease-modifying anti-rheumatic drug (DMARD). In the context of RA treatment, the use of modified-release prednisone formulations at night may offer the option of respecting circadian rhythms of both inflammatory response and HPA activation, thereby enabling low-dose GC administration to mitigate nocturnal inflammation and prolonged morning fatigue and joint stiffness. Long-term GC use should be individualized based on patient characteristics and minimized due to their potential AEs. Their chronic use, especially at medium/high dosages, might cause irreversible organ damage due to the burden of metabolic systemic effects and increased risk of infections. Many international guidelines recommend tapering/withdrawal of GCs in sustained remission. Treat-to-target (T2T) strategies are critical in setting targets for disease activity and reducing/discontinuing GCs once control is achieved.
Conclusions: Glucocorticosteroids' use in treating IRDs should be judicious, focused on minimizing use, tapering and discontinuing treatment, when possible, to improve long-term safety. Glucocorticosteroids remain part of many therapeutic regimens, particularly at low doses, and elderly RA patients, especially with associated chronic comorbidities, may benefit from long-term low-dose GC treatment. A personalized GC therapy is essential for optimal long-term outcomes.
Keywords: immune-mediated rheumatic diseases; overview on glucocorticosteroids; quality of life.
Copyright: © 2023 Narodowy Instytut Geriatrii, Reumatologii i Rehabilitacji w Warszawie.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous