

Overuse and underuse of thromboprophylaxis in medical inpatients
- PMID: 37745158
- PMCID: PMC10514554
- DOI: 10.1016/j.rpth.2023.102184
Overuse and underuse of thromboprophylaxis in medical inpatients
Abstract
Background: Thromboprophylaxis (TPX) prescription is recommended in medical inpatients categorized as high risk of venous thromboembolism (VTE) by validated risk assessment models (RAMs), but how various RAMs differ in categorizing patients in risk groups, and whether the choice of RAM influences estimates of appropriate TPX use is unknown.
Objectives: To determine the proportion of medical inpatients categorized as high or low risk according to validated RAMs, and to investigate the appropriateness of TPX prescription.
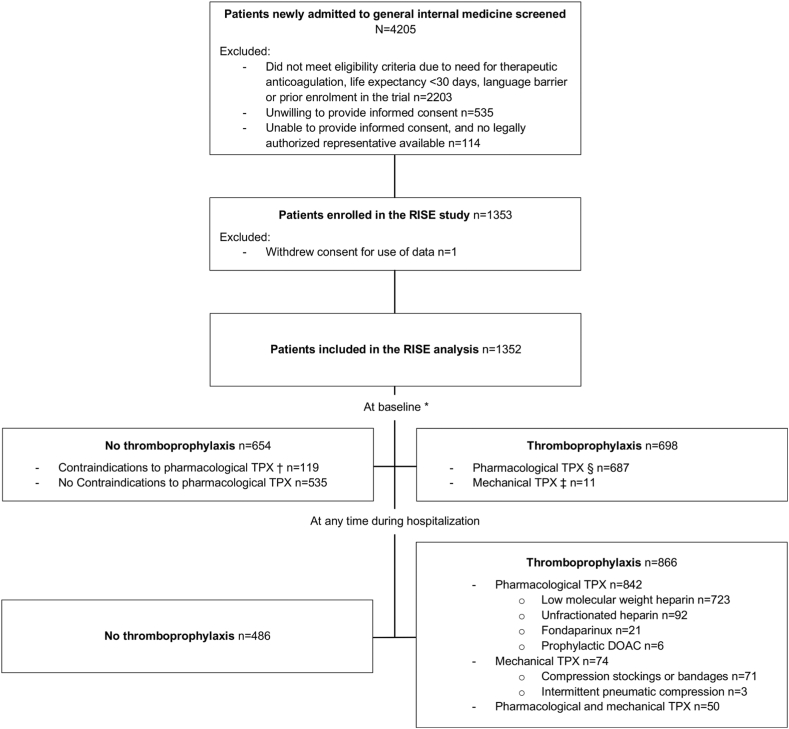
Methods: This is a prospective cohort study of acutely ill medical inpatients from 3 Swiss university hospitals. Participants were categorized as high or low risk of VTE by validated RAMs (ie, the Padua, the International Medical Prevention Registry on Venous Thromboembolism, simplified, and original Geneva scores). We assessed prescription of any TPX at baseline. We considered TPX prescription in high-risk and no TPX prescription in low-risk patients as appropriate.
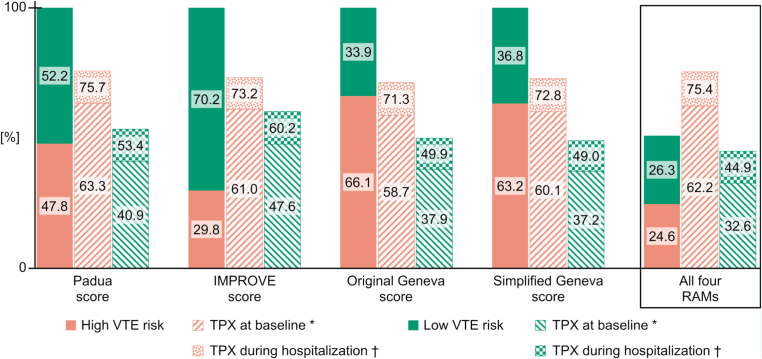
Results: Among 1352 medical inpatients, the proportion categorized as high risk ranged from 29.8% with the International Medical Prevention Registry on Venous Thromboembolism score to 66.1% with the original Geneva score. Overall, 24.6% were consistently categorized as high risk, and 26.3% as low risk by all 4 RAMs. Depending on the RAM used, TPX prescription was appropriate in 58.7% to 63.3% of high-risk (ie, 36.7%-41.3% underuse) and 52.4% to 62.8% of low-risk patients (ie, 37.2%-47.6% overuse).
Conclusion: The proportion of medical inpatients considered as high or low VTE risk varied widely according to different RAMs. Only half of patients were consistently categorized in the same risk group by all RAMs. While TPX remains underused in high-risk patients, overuse in low-risk patients is even more pronounced.
Keywords: hospitalization; prescriptions; prevention; prophylaxis; risk assessment; venous thromboembolism; venous thrombosis.
© 2023 The Author(s).
Figures
References
-
- Heit J.A., O’Fallon W.M., Petterson T.M., Lohse C.M., Silverstein M.D., Mohr D.N., et al. Relative impact of risk factors for deep vein thrombosis and pulmonary embolism: a population-based study. Arch Intern Med. 2002;162:1245–1248. - PubMed
-
- Heit J.A. Venous thromboembolism epidemiology: implications for prevention and management. Semin Thromb Hemost. 2002;28:3–13. - PubMed
-
- Falck-Ytter Y., Francis C.W., Johanson N.A., Curley C., Dahl O.E., Schulman S., et al. Prevention of VTE in orthopedic surgery patients: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012;141:e278S–e325S. - PMC - PubMed
-
- Goldhaber S.Z., Dunn K., MacDougall R.C. New onset of venous thromboembolism among hospitalized patients at Brigham and Women's Hospital is caused more often by prophylaxis failure than by withholding treatment. Chest. 2000;118:1680–1684. - PubMed
