

Cardiopulmonary interactions during ventilator weaning
- PMID: 37745230
- PMCID: PMC10512459
- DOI: 10.3389/fphys.2023.1275100
Cardiopulmonary interactions during ventilator weaning
Abstract
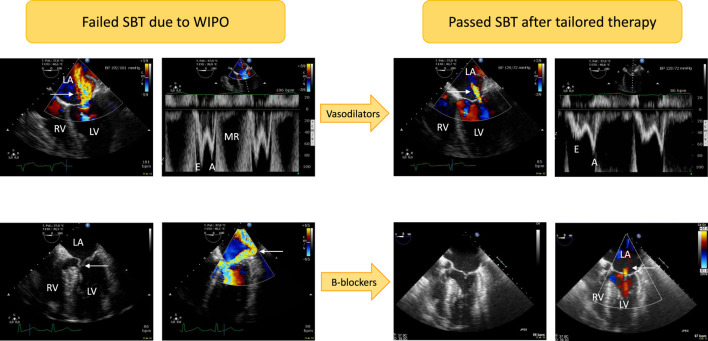
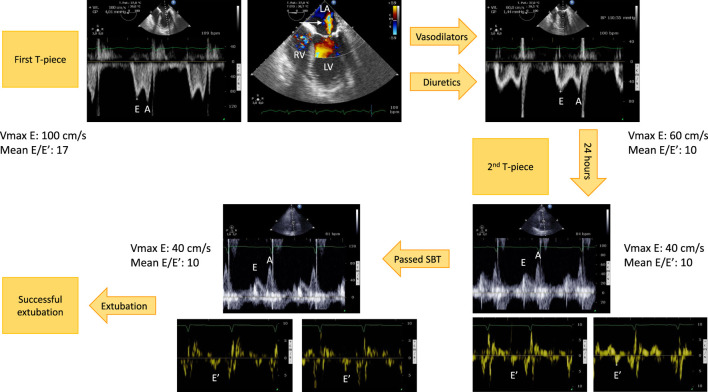
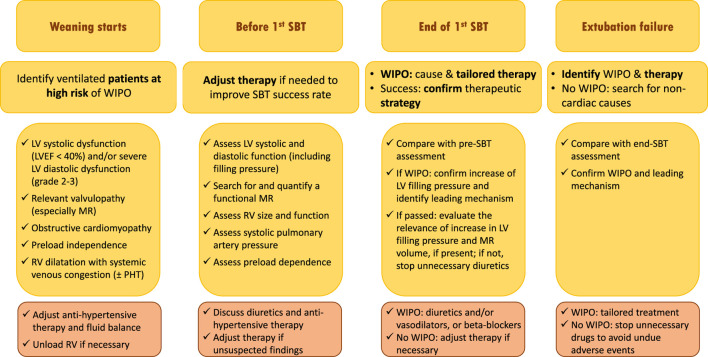
Weaning a critically-ill patient from the ventilator is a crucial step in global management. This manuscript details physiological changes induced by altered heart-lung interactions during the weaning process, illustrates the main mechanisms which could lead to weaning failure of cardiac origin, and discuss a tailored management based on the monitoring of changes in central hemodynamics during weaning. The transition from positive-pressure ventilation to spontaneous breathing results in abrupt hemodynamic and metabolic changes secondary to rapidly modified heart-lung interactions, sudden changes in cardiac loading conditions, and increased oxygen demand. These modifications may elicit an excessive burden on both the respiratory and cardiovascular systems, result in a rapid and marked increase of left ventricular filling pressure, and ultimately result in a weaning-induced pulmonary oedema (WIPO). The T-piece trial induces the greatest burden on respiratory and cardiocirculatory function when compared to spontaneous breathing trial using pressure support ventilation with positive or zero end-expiratory pressure. Since LV overload is the mainstay of WIPO, positive fluid balance and SBT-induced acute hypertension are the most frequently reported mechanisms of weaning failure of cardiac origin. Although the diagnosis of WIPO historically relied on an abrupt elevation of pulmonary artery occlusion pressure measured during right heart catheterization, it is nowadays commonly documented by echocardiography Doppler. This non-invasive approach is best suited for identifying high-risk patients, depicting the origin of WIPO, and tailoring individual management. Whether this strategy increases the success rate of weaning needs to be evaluated in a population at high risk of weaning failure of cardiac origin.
Keywords: echocardiography; heart-lung interactions; mechanical ventilation; pulmonary edema; weaning.
Copyright © 2023 Vignon.
Conflict of interest statement
The author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources