

Cervical muscle morphometry and composition demonstrate prognostic value in degenerative cervical myelopathy outcomes
- PMID: 37745653
- PMCID: PMC10512835
- DOI: 10.3389/fneur.2023.1209475
Cervical muscle morphometry and composition demonstrate prognostic value in degenerative cervical myelopathy outcomes
Abstract
Objectives: This study aimed to examine whether preoperative cervical muscle size, composition, and asymmetry from magnetic resonance imaging (MRI) can predict post-operative outcomes in patients with degenerative cervical myelopathy (DCM).
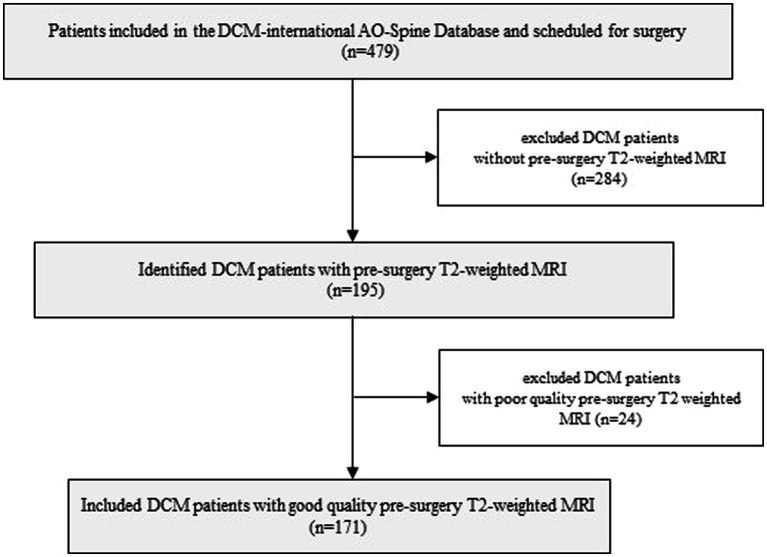
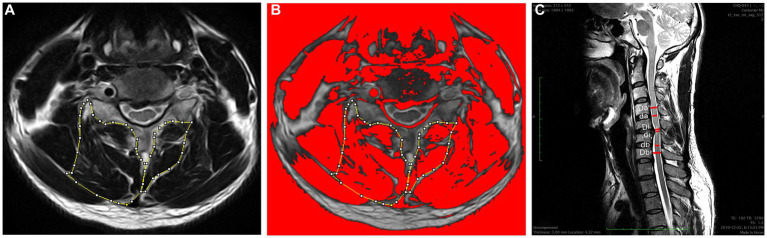
Methods: A total of 171 patients with DCM were included. Relative total cross-sectional area (RCSA), functional CSA (fat-free area, FCSA), ratio of FCSA/CSA (fatty infiltration) and asymmetry of the multifidus (MF) and semispinalis cervicis (SCer) together (MF + SCer), and cervical muscle as a group (MF, SCer, semispinalis capitis, and splenius capitis) were obtained from T2-weighted axial MR images at the mid-disk, at the level of maximum cord compression and the level below. Univariate and multivariate linear regression analyses were used to assess the relationship between baseline cervical muscle measurements of interest with the modified Japanese Orthopedic Association (mJOA), Nurick Classification, Neck Disability Index (NDI), and SF-36 health survey at 6-month and 12-month post-surgery.
Results: Lower RCSA of MF + SCer, less CSA MF + SCer asymmetry and greater FCSA/CSA for the cervical muscle group (e.g., less fatty infiltration), and younger age were significant predictors of higher mJOA scores (e.g., less disability) at 6-month and 12-month post-surgery (all p < 0.05). Greater CSA asymmetry in MF + SCer and lower FCSA/CSA (e.g., more fatty infiltration) for the cervical muscle group were significant predictors of higher Nurick scores (e.g., more disability) at 6-month and 12-month post-surgery (all p < 0.05). Lower FCSA MF + Scer asymmetry, lower FCSA/CSA asymmetry of the muscle group, and greater RCSA MF + SCer were significant predictors of higher NDI scores at 6-month and 12-month post-surgery. Finally, greater FCSA/CSA asymmetry of the MF + SCer, greater FCSA asymmetry of the muscle group, greater RCSA of the muscle group, and greater CSA asymmetry of MF + SCer were significant predictors of lower post-operative SF-36 scores at 6- and 12-month post-surgery.
Conclusion: Our result suggested that cervical paraspinal muscle morphology, specifically greater asymmetry, and fatty infiltration may be important predictors of functional recovery and post-surgical outcomes in patients with DCM.
Keywords: cervical extensor muscles composition; cervical extensor muscles morphology; degenerative cervical myelopathy; magnetic resonance imaging; post-operative outcome.
Copyright © 2023 Naghdi, Elliott, Weber, Fehlings and Fortin.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Nakashima H, Tetreault LA, Nagoshi N, Nouri A, Kopjar B, Arnold PM, et al. . Does age affect surgical outcomes in patients with degenerative cervical myelopathy? Results from the prospective multicenter AOSpine international study on 479 patients. J Neurol Neurosurg Psychiatry. (2016) 87:734–40. doi: 10.1136/jnnp-2015-311074, PMID: - DOI - PMC - PubMed
-
- Singh A, Tetreault L, Casey A, Laing R, Statham P, Fehlings MG. A summary of assessment tools for patients suffering from cervical spondylotic myelopathy: a systematic review on validity, reliability and responsiveness. Eur Spine J. (2015) 24:209–28. doi: 10.1007/s00586-013-2935-x, PMID: - DOI - PubMed
LinkOut - more resources
Full Text Sources