What is the current status of primary care in the diagnosis and treatment of patients with vertigo and dizziness in Switzerland? A national survey
- PMID: 37745663
- PMCID: PMC10513417
- DOI: 10.3389/fneur.2023.1254080
What is the current status of primary care in the diagnosis and treatment of patients with vertigo and dizziness in Switzerland? A national survey
Abstract
Background: Vertigo and dizziness are among the most frequent presenting symptoms in the primary care physicians' (PCPs) office. With patients facing difficulties in describing their complaints and clinical findings often being subtle and transient, the diagnostic workup of the dizzy patient remains challenging. We aimed to gain more insights into the current state of practice in order to identify the limitations and needs of the PCPs and define strategies to continuously improve their knowledge in the care of the dizzy patient.
Materials and methods: Board-certified PCPs working in Switzerland were invited to participate in an online survey. A descriptive statistical analysis was performed, and prospectively defined hypotheses were assessed using regression analyses.
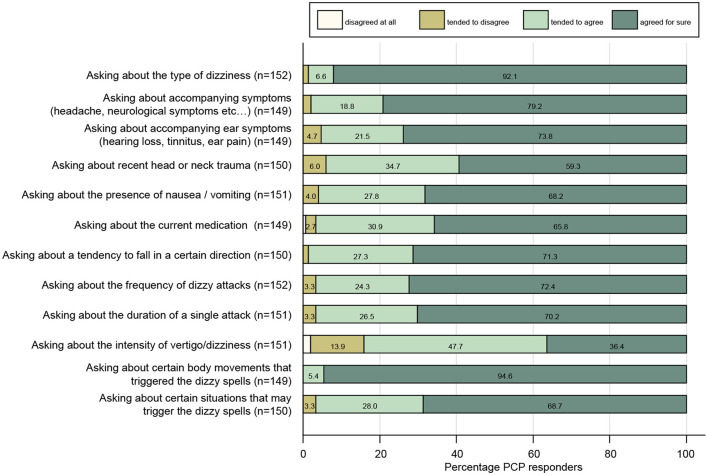
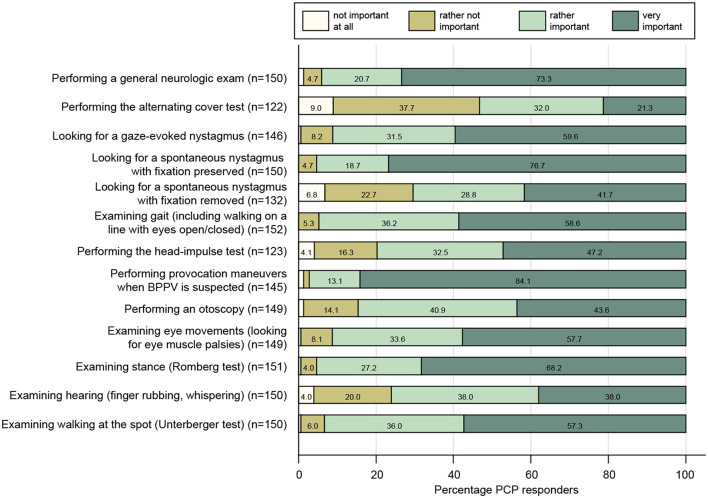
Results: A vast majority of participating PCPs (n = 152) were familiar with the key questions when taking the dizzy patient's history and with performing provocation/repositioning maneuvers when posterior-canal benign paroxysmal positional vertigo (BPPV) was suspected (91%). In contrast, strong agreement that performing the alternating cover test (21%), looking for a spontaneous nystagmus with fixation removed (42%), and performing the head-impulse test (47%) were important was considerably lower, and only 19% of PCPs were familiar with lateral-canal BPPV treatment. No specific diagnosis could be reached in substantial fractions of patients with acute (35% [25; 50%], median [inter-quartile range]) and episodic/chronic (50% [40; 65.8%]) dizziness/vertigo. Referral to specialists was higher in patients with episodic/chronic dizziness than in acutely dizzy patients (50% [20.3; 75] vs. 30% [20; 50]), with younger PCPs (aged 30-40 years) demonstrating significantly increased odds of referral to specialists (odds ratio = 2.20 [1.01-4.81], p = 0.048).
Conclusion: The assessment of dizzy patients takes longer than that of average patients in most primary care practices. Many dizzy patients remain undiagnosed even after a thorough examination, highlighting the challenges faced by PCPs and potentially leading to frequent referrals to specialists. To address this, it is crucial to promote state-of-the-art neuro-otological examination and treatment techniques that are currently neglected by most PCPs, such as "HINTS" and lateral-canal BPPV treatment. This can help reduce referral rates allowing more targeted treatment and referrals.
Keywords: bedside examination; diagnosis; dizziness; primary care; survey; vertigo.
Copyright © 2023 Zwergal, Mantokoudis, Heg, Kerkeni, Diener, Kalla, Korda, Candreia, Welge-Lüssen and Tarnutzer.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures