

The Added Value of Preprocedural Cardiac Computed Tomography in Planning Left Atrial Appendage Closure With the Watchman FLX Device
- PMID: 37745676
- PMCID: PMC10513000
- DOI: 10.1016/j.shj.2023.100188
The Added Value of Preprocedural Cardiac Computed Tomography in Planning Left Atrial Appendage Closure With the Watchman FLX Device
Abstract
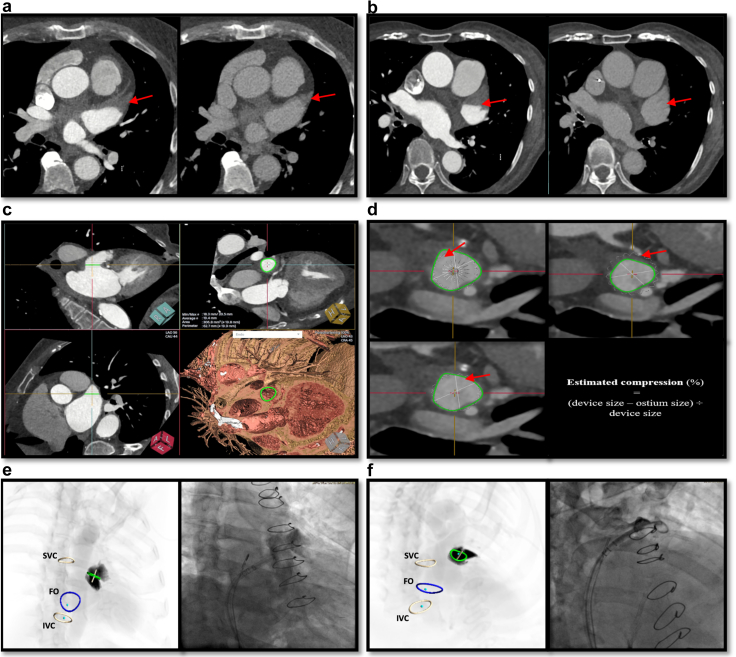
•Cardiac computed tomography (CCT) can be used as a useful complementary tool in preprocedural planning of left atrial appendage closure.•CCT planning includes assessing exclusion criteria, device sizing, sheath selection, anticipating challenging anatomies, and transseptal puncture planning.•Procedural 3D intracardiac echocardiography (3D-ICE) is increasingly being used instead of transesophageal echocardiography. In this setting, preprocedural CCT is useful to compensate for 3D ICE's reduced resolution.
Keywords: Cardiac computed tomography; Intracardiac echocardiography; Left atrial appendage closure; Preprocedural planning; Transesophageal echocardiography.
© 2023 The Authors.
Conflict of interest statement
Serge C. Harb is on the advisory board for TruPlan and a consultant/speaker for Boston Scientific. The other authors had no conflicts to declare.
Figures




References
-
- Troupis J., Crossett M., Scneider-Kolsky M., Nandurkar D. Presence of accessory left atrial appendage/diverticula in a population with atrial fibrillation compared with those in sinus rhythm: a retrospective review. Int J Cardiovasc Imaging. 2012;28:375–380. - PubMed
-
- Nagai T., Fujii A., Nishimura K., et al. Large thrombus originating from left atrial diverticulum: a new concern for catheter ablation of atrial fibrillation. Circulation. 2011;124:1086–1088. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
