

Case report: a premature infant with severe intrauterine growth restriction, adrenal insufficiency, and inflammatory diarrhea: a genetically confirmed case of MIRAGE syndrome
- PMID: 37745698
- PMCID: PMC10516543
- DOI: 10.3389/fendo.2023.1242387
Case report: a premature infant with severe intrauterine growth restriction, adrenal insufficiency, and inflammatory diarrhea: a genetically confirmed case of MIRAGE syndrome
Abstract
Introduction: MIRAGE syndrome is a rare disease characterized by myelodysplasia, infection, growth restriction, adrenal hypoplasia, genital phenotypes, and enteropathy. Herein, we report the case of a girl with MIRAGE syndrome who presented with adrenal insufficiency and chronic diarrhea.
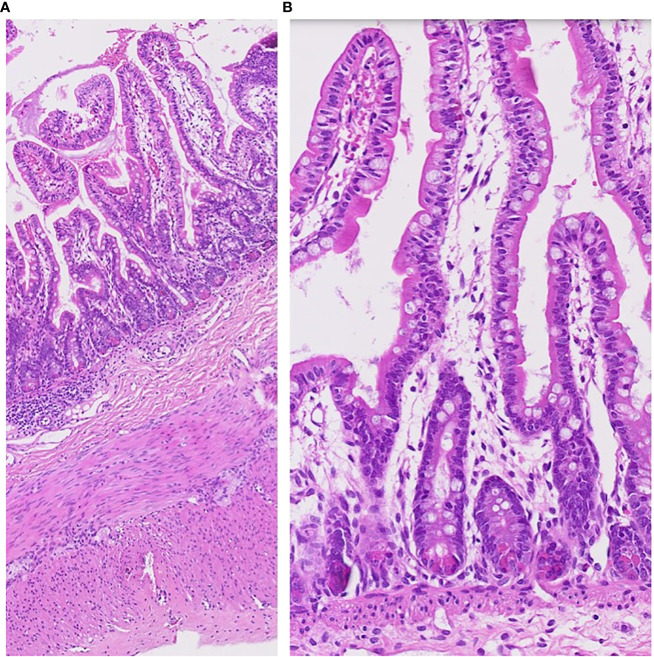
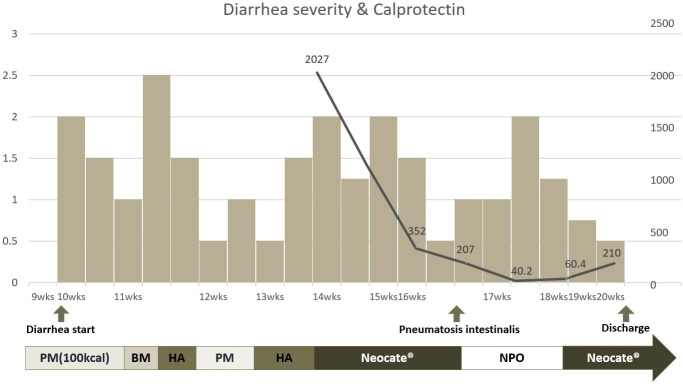
Case presentation: The patient was born at 29 + 6 weeks of gestational age with a birth weight of 656 g (<3p). Her height and head circumference were also <3p. At birth, she presented with respiratory distress, meconium staining, and pneumomediastinum, which were managed with high-frequency ventilation and empirical antibiotics. Physical examination showed generalized hyperpigmentation and normal female genitalia. A few days after birth, polyuria and hypotension developed, and laboratory findings revealed hypoglycemia, hyponatremia, and hyperkalemia. Plasma adrenocorticotropic hormone levels were elevated with low serum cortisol levels and high plasma renin activity, which were suggestive of adrenal insufficiency. Hydrocortisone and fludrocortisone were introduced and maintained, and hyperpigmentation attenuated with time. Both kidneys looked dysplastic, and adrenal glands could not be traced on abdominal ultrasound. From the early days of life, thrombocytopenia and anemia were detected, but not to life-threatening level and slowly recovered up to the normal range. Despite aggressive nutritional support, weight gain and growth spurt were severely retarded during the hospital stay. Additionally, after introducing enteral feeding, she experienced severe diarrhea and subsequent perineal skin rashes and ulcerations. Fecal calprotectin level was highly elevated; however, a small bowel biopsy resulted in non-specific submucosal congestion. The patient was diagnosed with MIRAGE syndrome with SAMD9 gene mutation. She was discharged with tube feeding and elemental formula feeding continued, but chronic diarrhea persisted. By the time of the last follow-up at 15 months of corrected age, she was fortunately not subjected to severe invasive infection and myelodysplastic syndrome. However, she was dependent on tube feeding and demonstrated a severe developmental delay equivalent to approximately 5-6 months of age.
Conclusion: The early diagnosis of adrenal crisis and hormone replacement therapy can save the life of -patients with MIRAGE syndrome; however, chronic intractable diarrhea and growth and developmental delay continue to impede the patient's well-being.
Keywords: MIRAGE syndrome; SAMD9; adrenal insufficiency (AI); enteropathy; hypoplasia.
Copyright © 2023 Go, Lee, Choi, Jeong, Jung and Lee.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures


References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical