

Reproducibility of Rejection Grading in Uterus Transplantation: A Multicenter Study
- PMID: 37745947
- PMCID: PMC10513355
- DOI: 10.1097/TXD.0000000000001535
Reproducibility of Rejection Grading in Uterus Transplantation: A Multicenter Study
Abstract
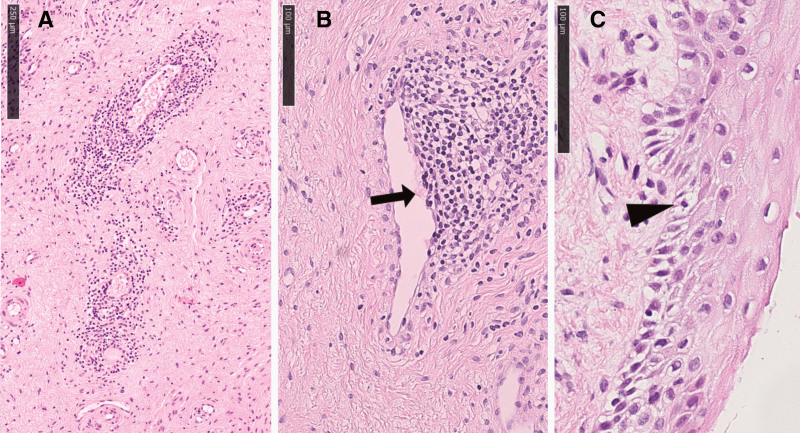
Background: Diagnosis of rejection after uterus transplantation is based on histopathological examination of ectocervical biopsies. Inflammation at the stromal-epithelial interface is the backbone of the histopathological classification proposed by our group in 2017. However, the reproducibility of this grading scheme has not been tested, and it is unclear whether it covers the full morphological spectrum of rejection.
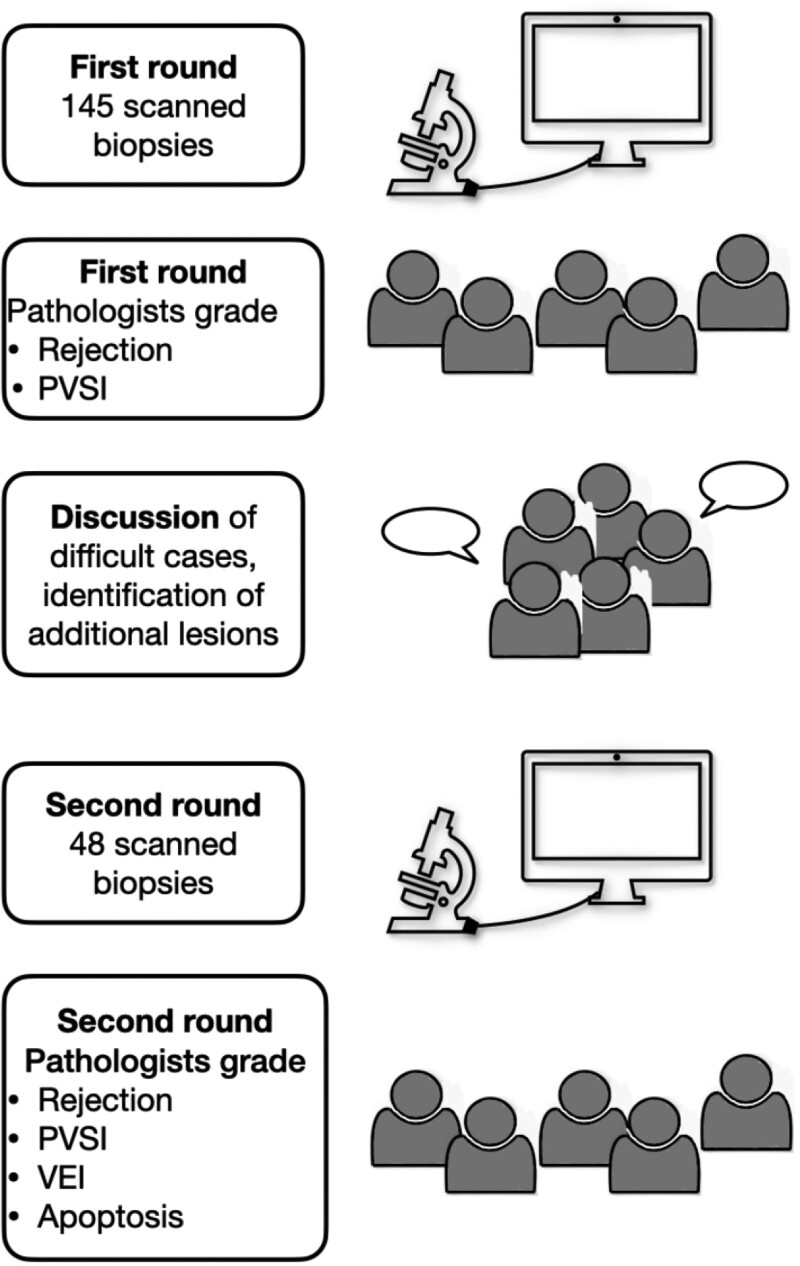
Methods: We present a multicenter study in which 5 pathologists from 4 uterus transplantation centers performed 2 rounds of grading on 145 and 48 cervical biopsies, respectively. Three of the centers provided biopsies. Additionally, the presence of perivascular stromal inflammation was recorded. During discussions after the first round, further histological lesions (venous endothelial inflammation and apoptosis) were identified for closer evaluation and added to the panel of lesions to score in the second round. All participants completed a questionnaire to explore current practices in handling and reporting uterus transplant biopsies.
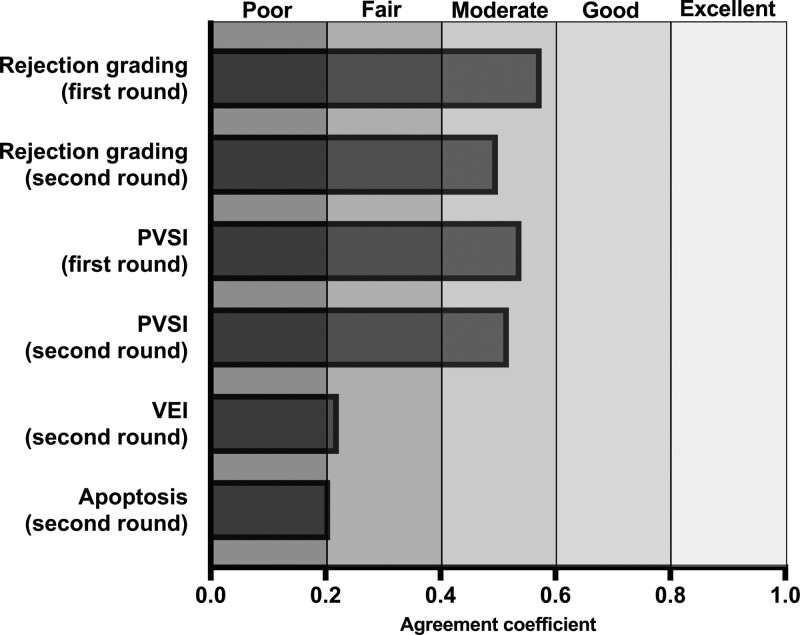
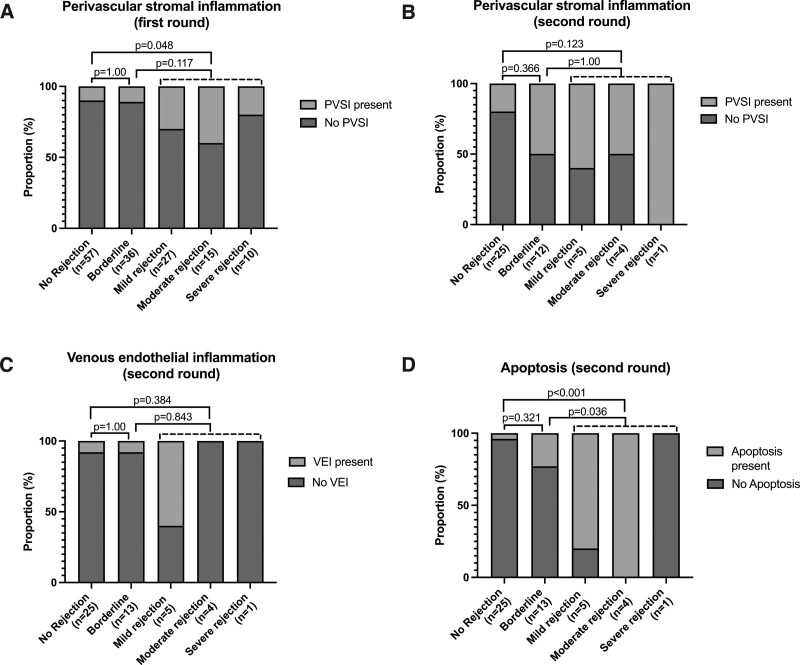
Results: Cervical biopsies were commonly performed in all centers to monitor rejection. Intraobserver reproducibility of rejection grading (performed by 1 rater) was excellent, whereas interobserver reproducibility was moderate and did not improve in the second round. Reproducibility of perivascular stromal inflammation was moderate but unsatisfactory for venous endothelial inflammation and apoptosis. All lesions were more frequent in, but not restricted to, biopsies with rejection patterns.
Conclusions: Grading of rejection in cervical biopsies is reproducible and applicable to biopsies from different centers. Diagnosis of rejection may be improved by adding further histological lesions to the grading system; however, lesions require rigorous consensus definition.
Copyright © 2023 The Author(s). Transplantation Direct. Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Transcript analysis of uterus transplant cervical biopsies using the Banff Human Organ Transplant panel.Am J Transplant. 2025 Feb;25(2):329-342. doi: 10.1016/j.ajt.2024.08.027. Epub 2024 Aug 30. Am J Transplant. 2025. PMID: 39216690
-
Histopathological examination of the ectocervical biopsy in non-transplanted uteri: A study contributing to the provisional scoring system of subclinical graft rejection after uterus transplantation.Acta Obstet Gynecol Scand. 2022 Jan;101(1):37-45. doi: 10.1111/aogs.14280. Epub 2021 Oct 25. Acta Obstet Gynecol Scand. 2022. PMID: 34693986 Free PMC article.
-
Reliability and predictive value of the National Institute of Diabetes and Digestive and Kidney Diseases Liver Transplantation Database nomenclature and grading system for cellular rejection of liver allografts.Hepatology. 1995 Feb;21(2):408-16. Hepatology. 1995. PMID: 7843714 Clinical Trial.
-
Banff schema for grading pancreas allograft rejection: working proposal by a multi-disciplinary international consensus panel.Am J Transplant. 2008 Jun;8(6):1237-49. doi: 10.1111/j.1600-6143.2008.02212.x. Epub 2008 Apr 29. Am J Transplant. 2008. PMID: 18444939
-
Revision of the 1996 working formulation for the standardization of nomenclature in the diagnosis of lung rejection.J Heart Lung Transplant. 2007 Dec;26(12):1229-42. doi: 10.1016/j.healun.2007.10.017. J Heart Lung Transplant. 2007. PMID: 18096473
References
-
- Herlin M, Bjorn AM, Rasmussen M, et al. . Prevalence and patient characteristics of Mayer-Rokitansky-Küster-Hauser syndrome: a nationwide registry-based study. Hum Reprod. 2016;31:2384–2390. - PubMed
-
- Brannstrom M, Belfort MA, Ayoubi JM. Uterus transplantation worldwide: clinical activities and outcomes. Curr Opin Organ Transplant. 2021;26:616–626. - PubMed
-
- Stewart S, Winters GL, Fishbein MC, et al. . Revision of the 1990 working formulation for the standardization of nomenclature in the diagnosis of heart rejection. J Heart Lung Transplant. 2005;24:1710–1720. - PubMed
-
- Cendales LC, Kanitakis J, Schneeberger S, et al. . The Banff 2007 working classification of skin-containing composite tissue allograft pathology. Am J Transplant. 2008;8:1396–1400. - PubMed
LinkOut - more resources
Full Text Sources
Medical
