

Fibrinolytic potential as a risk factor for postpartum hemorrhage
- PMID: 37746089
- PMCID: PMC10516290
- DOI: 10.3389/fmed.2023.1208103
Fibrinolytic potential as a risk factor for postpartum hemorrhage
Abstract
Background: Postpartum hemorrhage (PPH) is still the leading cause of maternal morbidity and mortality worldwide. While impaired fibrin polymerization plays a crucial role in the development and progress of PPH, recent approaches using viscoelastic measurements have failed to sensitively detect early changes in fibrinolysis in PPH. This study aimed to evaluate whether women experiencing PPH show alterations in POC-VET fibrinolytic potential during childbirth and whether fibrinolytic potential offers benefits in the prediction and treatment of PPH.
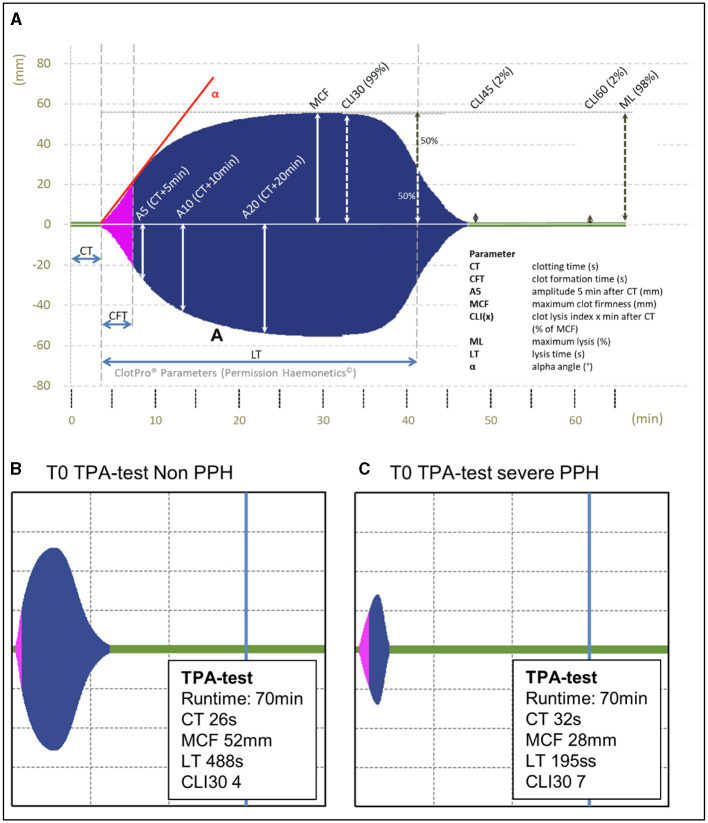
Methods: Blood samples were collected at three different timepoints: T0 = hospital admission (19 h ± 18 h prepartum), T1 = 30-60 min after placental separation, and T2 = first day postpartum (19 h ± 6 h postpartum). In addition to standard laboratory tests, whole-blood impedance aggregometry (Multiplate) and viscoelastic testing (VET) were performed using the ClotPro system, which included the TPA-test lysis time, to assess the POC-VET fibrinolytic potential, and selected coagulation factors were measured. The results were correlated with blood loss and clinical outcome markers. Severe PPH was defined as a hemoglobin drop > 4g/dl and/or the occurrence of shock or the need for red blood cell transfusion.
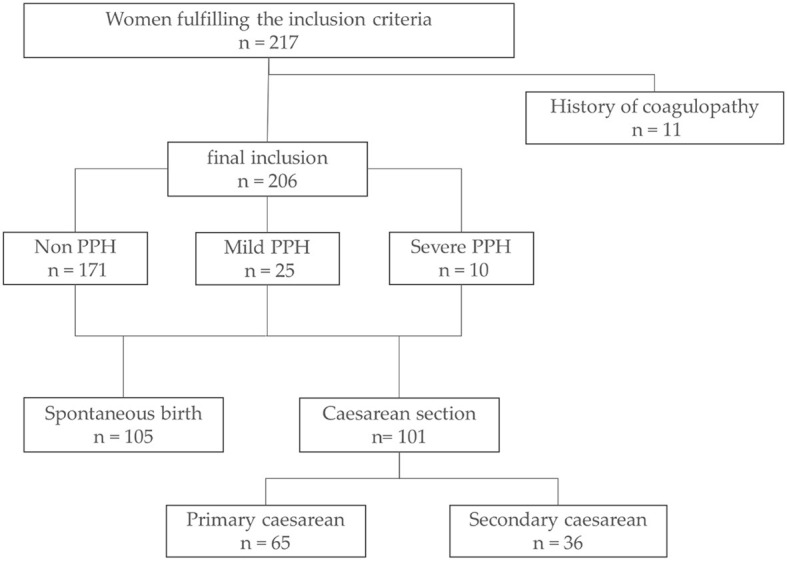
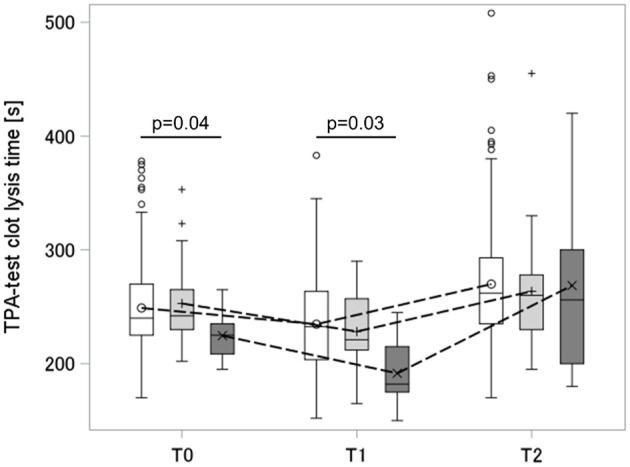
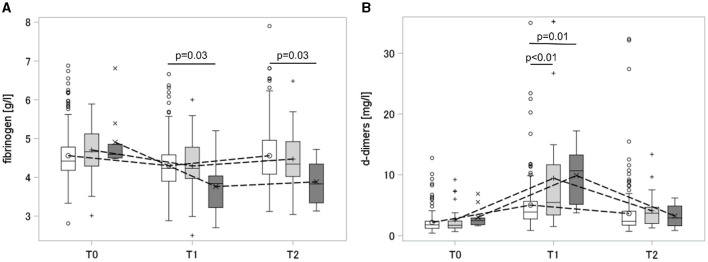
Results: Blood samples of 217 parturient women were analyzed between June 2020 and December 2020 at Heidelberg University Women's Hospital, and 206 measurements were eligible for the final analysis. Women experiencing severe PPH showed increased fibrinolytic potential already at the time of hospital admission. When compared to non-PPH, the difference persisted 30-60 min after placental separation. A higher fibrinolytic potential was accompanied by a greater drop in fibrinogen and higher d-dimer values after placental separation. While 70% of women experiencing severe PPH showed fibrinolytic potential, 54% of those without PPH showed increased fibrinolytic potential as well.
Conclusion: We were able to show that antepartal and peripartal fibrinolytic potential was elevated in women experiencing severe PPH. However, several women showed high fibrinolytic potential but lacked clinical signs of PPH. The findings indicate that high fibrinolytic potential is a risk factor for the development of coagulopathy, but further conditions are required to cause PPH.
Keywords: ClotPro; PPH; TPA-test; VET; fibrinolytic potential; point-of-care; viscoelastic hemostatic assay.
Copyright © 2023 Gruneberg, Braun, Schöchl, Nachtigall-Schmitt, von der Forst, Tourelle, Dietrich, Wallwiener, Wallwiener, Weigand, Fluhr, Spratte, Hofer and Schmitt.
Conflict of interest statement
HS has received honoraria for participation in advisory board meetings for Alexion, Bayer Healthcare, Boehringer Ingelheim, Haemonetics and Vifor, and has received study grants and speaker's honorarium from CSL Behring. FS has received research support from CSL Behring and Philips, as well as speaker honorarium from CSL Behring and AstraZeneca and he is a consultant in an advisory board for CSL Behring. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. The authors declare that this study received funding from Enicor (consumables). The funder was not involved in the study design, collection, analysis, interpretation of data, the writing of this article or the decision to submit it for publication.
Figures
Similar articles
-
Point-of-care diagnosis and monitoring of fibrinolysis resistance in the critically ill: results from a feasibility study.Crit Care. 2023 Feb 10;27(1):55. doi: 10.1186/s13054-023-04329-5. Crit Care. 2023. PMID: 36765421 Free PMC article.
-
Predictive ability of viscoelastic testing using ClotPro® for short-term outcome in patients with severe Covid-19 ARDS with or without ECMO therapy: a retrospective study.Thromb J. 2022 Aug 29;20(1):48. doi: 10.1186/s12959-022-00403-0. Thromb J. 2022. PMID: 36038895 Free PMC article.
-
Aetiology and treatment of severe postpartum haemorrhage.Dan Med J. 2018 Mar;65(3):B5444. Dan Med J. 2018. PMID: 29510809 Review.
-
High prevalence of postpartum hemorrhage in women with rare bleeding disorders in the Netherlands: retrospective data from the RBiN study.J Thromb Haemost. 2023 Mar;21(3):499-512. doi: 10.1016/j.jtha.2022.11.009. Epub 2022 Dec 22. J Thromb Haemost. 2023. PMID: 36696205
-
Obstetric hemorrhage and coagulation: an update. Thromboelastography, thromboelastometry, and conventional coagulation tests in the diagnosis and prediction of postpartum hemorrhage.Obstet Gynecol Surv. 2012 Jul;67(7):426-35. doi: 10.1097/OGX.0b013e3182605861. Obstet Gynecol Surv. 2012. PMID: 22926249 Review.
Cited by
-
Association Between Laboratory Coagulation Parameters and Postpartum Hemorrhage in Preterm and Term Caesarean Section: A Retrospective Analysis.J Clin Med. 2024 Nov 3;13(21):6604. doi: 10.3390/jcm13216604. J Clin Med. 2024. PMID: 39518742 Free PMC article.
-
Comparison of Two Viscoelastic Testing Devices in a Parturient Population.J Clin Med. 2024 Jan 25;13(3):692. doi: 10.3390/jcm13030692. J Clin Med. 2024. PMID: 38337386 Free PMC article.
References
-
- Knight M, Callaghan WM, Berg C, Alexander S, Bouvier-Colle MH, Ford JB, et al. . Trends in postpartum hemorrhage in high resource countries: a review and recommendations from the International Postpartum Hemorrhage Collaborative Group. BMC Pregnancy Childbirth. (2009) 9:55. 10.1186/1471-2393-9-55 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources