

Correlation analysis of hemoglobin, albumin, lymphocyte, platelet score and platelet to albumin ratio and prognosis in patients with lung adenosquamous carcinoma
- PMID: 37746281
- PMCID: PMC10514357
- DOI: 10.3389/fonc.2023.1166802
Correlation analysis of hemoglobin, albumin, lymphocyte, platelet score and platelet to albumin ratio and prognosis in patients with lung adenosquamous carcinoma
Abstract
Objective: To investigate the effect of hemoglobin, albumin, lymphocytes, platelet (HALP) score and platelet to albumin ratio (PAR) on prognosis of patients with lung adenosquamous carcinoma (ASC) after surgery.
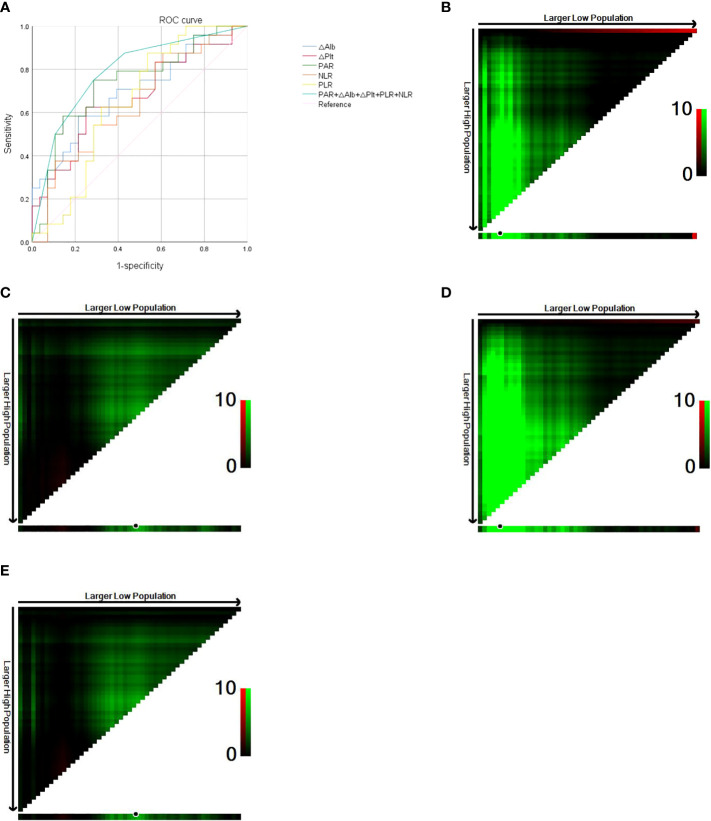
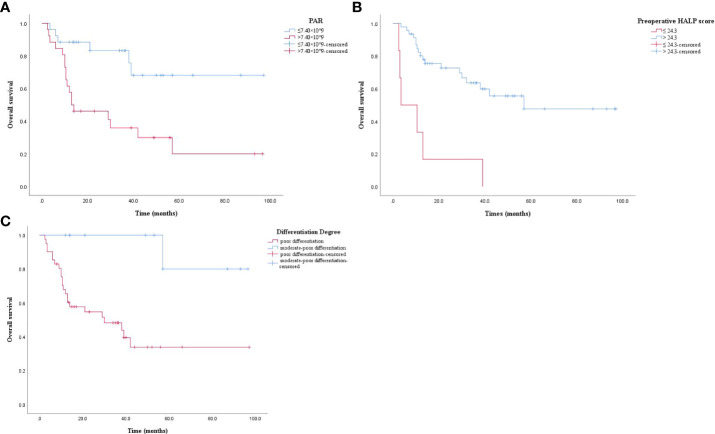
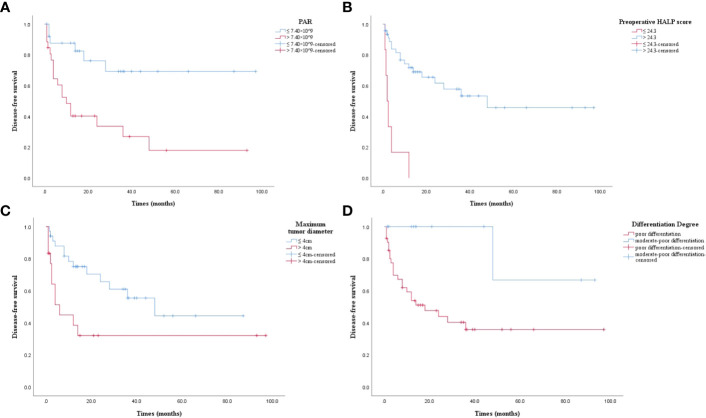
Patients and methods: A total of 52 patients diagnosed with ASC after surgical resection were collected from Nanjing Chest Hospital from 2012 to 2021, and their general clinical data, pathological data and laboratory indexes were collected. The changes of Alb and Plt levels before and after surgery, HALP scores (hemoglobin albumin lymphocytes/platelets), and postoperative PAR, PLR, NLR were retrospectively analyzed, and their influence on the prognosis of patients with ASC was investigated. The cut-off value of △Alb, △Plt, postoperative PAR, PLR and NLR were determined by the receiver operating characteristic (ROC) curve, the optimal cut-off value of HALP score before and after surgery was calculated by using X-tile software, and the clinicopathological characteristics were compared between the high PAR and low PAR groups and between high HALP score and low HALP score group to analyze the factors influencing the prognosis of patients with ASC. Univariate and multivariate Cox proportional regression analyses were used to assess independent risk factors affecting overall survival (OS) and disease-free survival (DFS) in patients with ASC. Kaplan-Meier method was used to evaluate the correlation between OS, DFS and PAR and HALP score.
Results: A critical value of PAR was 7.40×10^9 and an area under the curve (AUC) of 0.737 (95%CI: 0.597-0.876, P = 0.004). The best cut-off value of the preoperative HALP score was 24.3. Univariate Cox analysis showed that the cut margin (P = 0.013), the degree of differentiation (P = 0.021), N stage (P = 0.049), △Plt (P = 0.010), △Alb (P = 0.016), PAR (P = 0.003), NLR (P = 0.025), PLR (P = 0.029), preoperative HALP score (P = 0.000) and post-operative HALP score (P = 0.010) were all associated with postoperative OS in ASC patients. Cut margin (P = 0.029), the degree of differentiation (P = 0.045), maximum tumor diameter (P = 0.018), N stage (P = 0.035), △Plt (P = 0.007), △Alb (P = 0.007), PAR (P = 0.004), NLR (P = 0.041), PLR (P = 0.030), preoperative HALP score (P = 0.000), and postoperative HALP score (P = 0.011) were related to postoperative DFS in ASC patients. Multivariate analysis revealed that PAR (HR: 6.877, 95%CI: 1.817-26.038, P = 0.005), differentiation degree (HR: 0.059, 95%CI: 0.006-0.591, P = 0.016) and preoperative HALP score (HR: 0.224, 95%CI: 0.068-0.733, P = 0.013) had significant effect on OS. Tumor maximum diameter (HR: 3.442, 95%CI: 1.148-10.318, P = 0.027) and preoperative HALP score (HR: 0.268, 95%CI: 0.085-0.847, P = 0.025) had significant influence on DFS.
Conclusion: PAR and preoperative HALP score were potentially useful biomarkers for evaluating the outcome of patients with postoperative ASC. PAR, the degree of differentiation and preoperative HALP score were independent prognostic factors for postoperative OS in ASC patients. Maximum tumor diameter and preoperative HALP score were independent prognostic factors for postoperative DFS in ASC patients.
Keywords: HALP score; PAR; differentiation degree; lung adenosquamous carcinoma; prognosis; surgery.
Copyright © 2023 Zhang, Liu and Xu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
[Relationship between preoperative inflammatory indexes and prognosis of patients with rectal cancer and establishment of prognostic nomogram prediction model].Zhonghua Zhong Liu Za Zhi. 2022 May 23;44(5):402-409. doi: 10.3760/cma.j.cn112152-20200630-00612. Zhonghua Zhong Liu Za Zhi. 2022. PMID: 35615796 Chinese.
-
Hemoglobin, albumin, lymphocyte, and platelet score and neutrophil-to-lymphocyte ratio are novel significant prognostic factors for patients with small-cell lung cancer undergoing chemotherapy.J Cancer Res Ther. 2020 Sep;16(5):1134-1139. doi: 10.4103/jcrt.JCRT_1066_19. J Cancer Res Ther. 2020. PMID: 33004760
-
HALP score based on hemoglobin, albumin, lymphocyte and platelet can predict the prognosis of tongue squamous cell carcinoma patients.Heliyon. 2023 Sep 13;9(9):e20126. doi: 10.1016/j.heliyon.2023.e20126. eCollection 2023 Sep. Heliyon. 2023. PMID: 37809958 Free PMC article.
-
The preoperative hemoglobin, albumin, lymphocyte, and platelet score is a prognostic factor for non-small cell lung cancer patients undergoing adjuvant chemotherapy: a retrospective study.Ann Transl Med. 2022 Apr;10(8):457. doi: 10.21037/atm-22-1097. Ann Transl Med. 2022. PMID: 35571436 Free PMC article.
-
Prognostic significance of hemoglobin, albumin, lymphocyte and platelet score in solid tumors: a pooled study.Front Immunol. 2024 Dec 18;15:1483855. doi: 10.3389/fimmu.2024.1483855. eCollection 2024. Front Immunol. 2024. PMID: 39744624 Free PMC article.
Cited by
-
The prognostic and clinicopathological value of HALP score in non-small cell lung cancer.Front Immunol. 2025 Jun 26;16:1576326. doi: 10.3389/fimmu.2025.1576326. eCollection 2025. Front Immunol. 2025. PMID: 40642085 Free PMC article.
-
A nomogram model for predicting postoperative prognosis in patients with aneurysmal subarachnoid hemorrhage using preoperative biochemical indices.BMC Neurol. 2024 Aug 3;24(1):270. doi: 10.1186/s12883-024-03774-1. BMC Neurol. 2024. PMID: 39097679 Free PMC article.
-
Haemoglobin, albumin, lymphocyte, and platelet score as an independent predictor for renal prognosis in IgA nephropathy.Front Endocrinol (Lausanne). 2024 Apr 26;15:1339921. doi: 10.3389/fendo.2024.1339921. eCollection 2024. Front Endocrinol (Lausanne). 2024. PMID: 38737556 Free PMC article.
-
Neutrophil-to-lymphocyte ratio as a prognostic marker for lung cancer in combined pulmonary fibrosis and emphysema patients.Eur J Med Res. 2025 Apr 22;30(1):316. doi: 10.1186/s40001-025-02595-3. Eur J Med Res. 2025. PMID: 40264240 Free PMC article.
-
Association of hemoglobin, albumin, lymphocyte, and platelet score with all-cause and cardiovascular mortality in adults with diabetes or prediabetes: Results from NHANES 2005-2018.Prev Med Rep. 2025 May 5;54:103101. doi: 10.1016/j.pmedr.2025.103101. eCollection 2025 Jun. Prev Med Rep. 2025. PMID: 40469253 Free PMC article.
References
-
- Travis WD, Brambilla E, Nicholson AG, Yatabe Y, Austin JHM, Beasley MB, et al. . The 2015 world health organization classification of lung tumors: impact of genetic, clinical and radiologic advances since the 2004 classification. J Thorac Oncol (2015) 10(9):1243–60. doi: 10.1097/JTO.0000000000000630 - DOI - PubMed
-
- Maeda H, Matsumura A, Kawabata T, Suito T, Kawashima O, Watanabe T, et al. . Japan National Hospital Organization Study Group for Lung Cancer. Adenosquamous carcinoma of the lung: surgical results as compared with squamous cell and adenocarcinoma cases. Eur J Cardiothorac Surg (2012) 41(2):357–61. doi: 10.1016/j.ejcts.2011.05.050 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous