

Iatrogenic Thermal Energy-Induced Distal Ureteric Injury and Its Management by Laparoscopy Ureteroureterostomy
- PMID: 37746521
- PMCID: PMC10516262
- DOI: 10.4293/JSLS.2023.00030
Iatrogenic Thermal Energy-Induced Distal Ureteric Injury and Its Management by Laparoscopy Ureteroureterostomy
Abstract
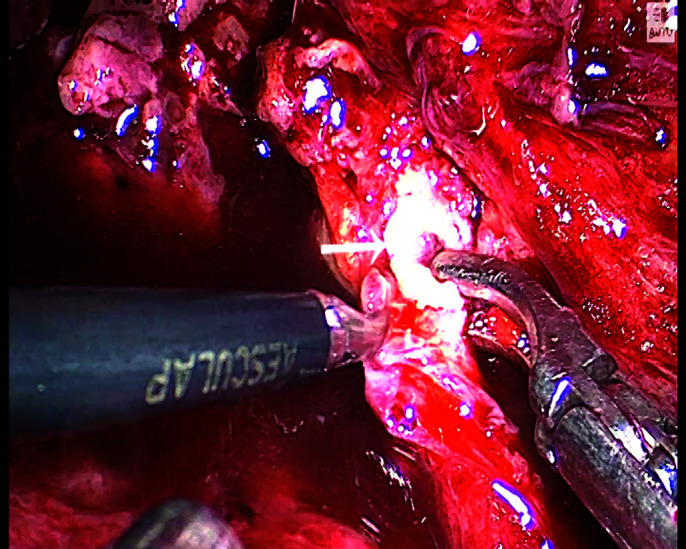
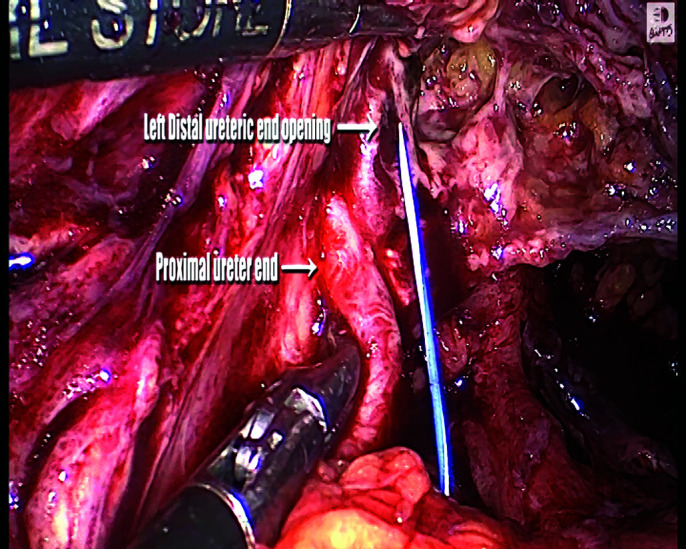
Background and objectives: Most thermal energy-induced distal ureter injuries are missed intraoperatively as they are caused by delayed ischemia-induced necrosis of the affected part leading to fistula, and a delayed presentation. The injuries of the distal ureter are commonly managed by ureteroneocystostomy, which has long-term complications related to vesico-ureteric reflux (VUR). We present our experience of management of distal ureter injury due to thermal energy by laparoscopy ureteroureterostomy and the role of various methodologies for its diagnosis.
Methods: It is a retrospective, single-center study that was conducted from January 1, 2020 - December, 31 2022.
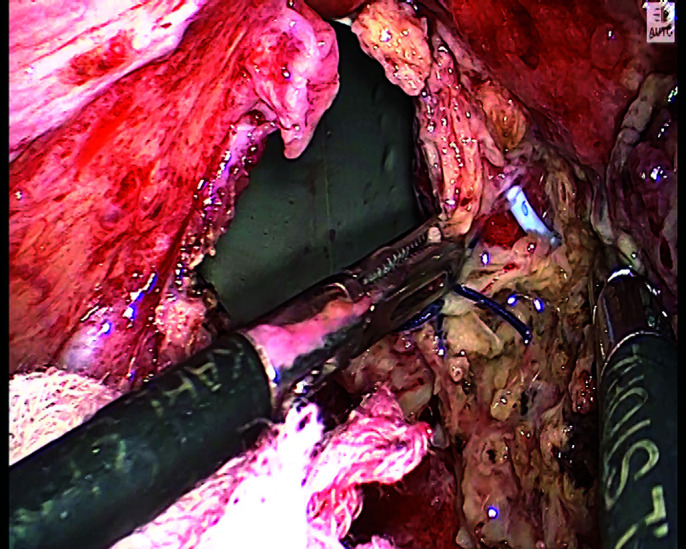
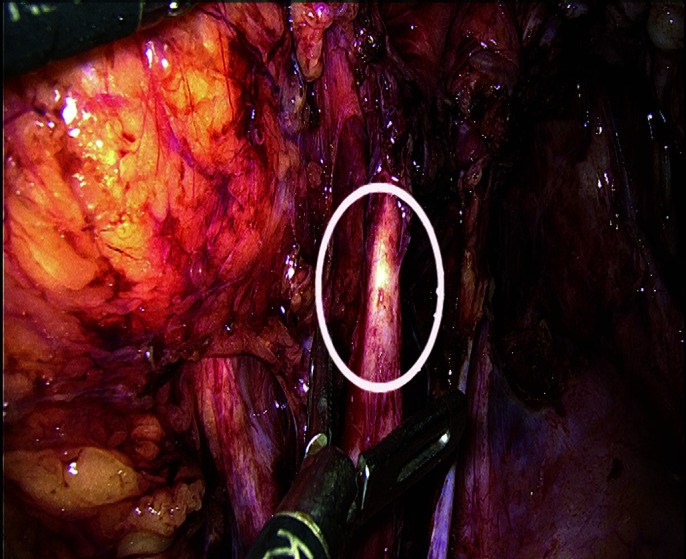
Results: A total of 8 cases were enrolled in the study. All cases had an uterovaginal fistula (UVF) post-laparoscopic gynecology surgery. The bilateral ureteric injury was observed in 2 cases. The median post-surgery time to diagnose UVF in the study was 10 days. All cases were managed by laparoscopy ureteroureterostomy (LUUS). Six cases underwent immediate surgery after the diagnosis; whereas 2 cases had initial double-J stent placement as treatment, which subsequently failed following which the LUUS was performed. There were not any immediate or long-term complications such as leakage, stenosis, fistula, or any requirement for revision surgery.
Conclusion: The management of thermal energy-induced ureteric injury is exceptional as compared to other types of ureteric injury. Our approach should be toward immediate surgical management rather than a conservative one to avoid long-term complications and sequelae. Iatrogenic lower ureteral injury can be managed successfully by LUUS, maintaining the normal anatomy and physiology of VUR.
Keywords: Double-J stent; Laparoscopy ureteroureterostomy; Reimplantation of the ureter; Thermal energy-induced ureter injury; Uretero-vaginal fistula; Vesico-ureter reflux.
© 2023 by SLS, Society of Laparoscopic & Robotic Surgeons.
Conflict of interest statement
Conflict of interests: none.
Figures




Similar articles
-
Iatrogenic ureteral injury during retroperitoneal laparoscopy for large renal cysts: What we learned and a review of the literature.J Xray Sci Technol. 2021;29(1):185-196. doi: 10.3233/XST-200804. J Xray Sci Technol. 2021. PMID: 33459688 Review.
-
[Post-hysterectomy uretero-vaginal fistula: Laparoscopic management with ureteroneocystostomy and psoas hitch.].Arch Esp Urol. 2019 May;72(4):428-435. Arch Esp Urol. 2019. PMID: 31070140 Review. Spanish.
-
Laparoscopic ureteroureterostomy with an intraoperative retrograde ureteroscopy-assisted technique for distal ureteral injury secondary to gynecological surgery: a retrospective comparison with laparoscopic ureteroneocystostomy.Scand J Urol. 2017 Aug;51(4):329-334. doi: 10.1080/21681805.2017.1304989. Epub 2017 Apr 7. Scand J Urol. 2017. PMID: 28388304
-
Outcome of laparoscopic repair of ureteral injury: follow-up of twelve cases.J Minim Invasive Gynecol. 2012 Jan-Feb;19(1):68-75. doi: 10.1016/j.jmig.2011.09.011. Epub 2011 Nov 18. J Minim Invasive Gynecol. 2012. PMID: 22100442
-
Management of postoperatively detected iatrogenic lower ureteral injury: should ureteroureterostomy really be abandoned?Urology. 2006 Feb;67(2):237-41. doi: 10.1016/j.urology.2005.08.041. Epub 2006 Jan 25. Urology. 2006. PMID: 16442604
Cited by
-
Dexamethasone: a cheap and convenient way to alleviate subsequent stenosis after thermal injury on ureter.Transl Androl Urol. 2024 Nov 30;13(11):2498-2509. doi: 10.21037/tau-24-343. Epub 2024 Nov 28. Transl Androl Urol. 2024. PMID: 39698563 Free PMC article.
-
Surgical Anatomical Structure of Uterine Artery Caudal Space for Robot-Assisted Extrafascial Hysterectomy With Ureterohypogastric Nerve Fascia Preservation: A Case Description.Cureus. 2024 Feb 20;16(2):e54512. doi: 10.7759/cureus.54512. eCollection 2024 Feb. Cureus. 2024. PMID: 38516437 Free PMC article.
References
-
- Wong JMK, Bortoletto P, Tolentino J, Jung MJ, Milad MP. Urinary tract injury in gynecologic laparoscopy for benign indication: a systematic review. Obstet Gynecol. 2018;131(1):100–108. - PubMed
-
- Vakili B, Chesson RR, Kyle BL, et al. The incidence of urinary tract injury during hysterectomy: a prospective analysis based on universal cystoscopy. Am J Obstet Gynecol. 2005;192(5):1599–1604. - PubMed
-
- Dallas KB, Rogo-Gupta L, Elliott CS. Urologic injury and fistula after hysterectomy for benign indications. Obstet Gynecol. 2019;134(2):241–249. - PubMed
-
- Parpala-Spårman T, Paananen I, Santala M, Ohtonen P, Hellström P. Increasing numbers of ureteric injuries after the introduction of laparoscopic surgery. Scand J Urol Nephrol. 2008;42(5):422–427. - PubMed
-
- Selli C, Turri FM, Gabellieri C, Manassero F, De Maria M, Mogorovich A. Delayed-onset ureteral lesions due to thermal energy: an emerging condition. Arch Ital Urol Androl. 2014;86(2):152–153. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical