

Early surgery versus conservative treatment in patients with traumatic intracerebral hematoma: a CENTER-TBI study
- PMID: 37747570
- PMCID: PMC10624744
- DOI: 10.1007/s00701-023-05797-y
Early surgery versus conservative treatment in patients with traumatic intracerebral hematoma: a CENTER-TBI study
Abstract
Purpose: Evidence regarding the effect of surgery in traumatic intracerebral hematoma (t-ICH) is limited and relies on the STITCH(Trauma) trial. This study is aimed at comparing the effectiveness of early surgery to conservative treatment in patients with a t-ICH.
Methods: In a prospective cohort, we included patients with a large t-ICH (< 48 h of injury). Primary outcome was the Glasgow Outcome Scale Extended (GOSE) at 6 months, analyzed with multivariable proportional odds logistic regression. Subgroups included injury severity and isolated vs. non-isolated t-ICH.
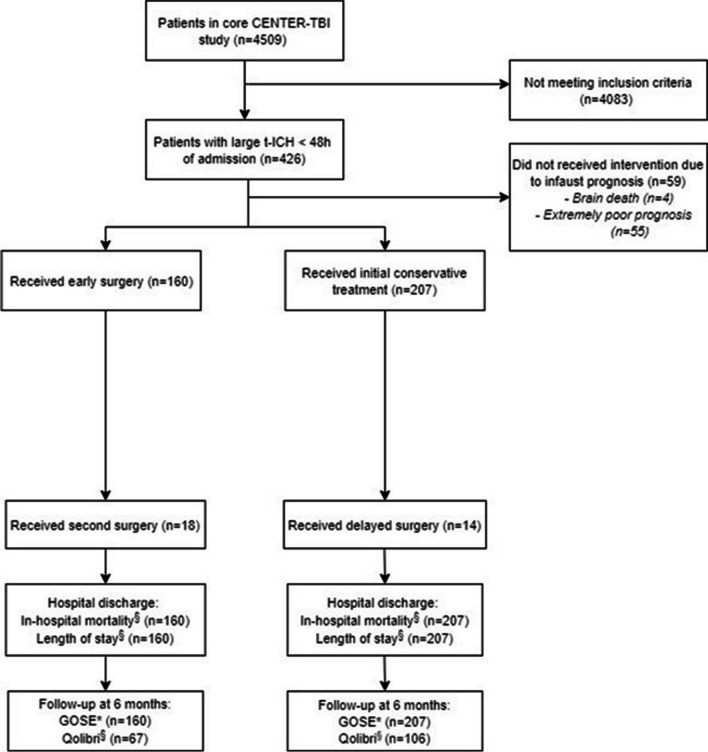
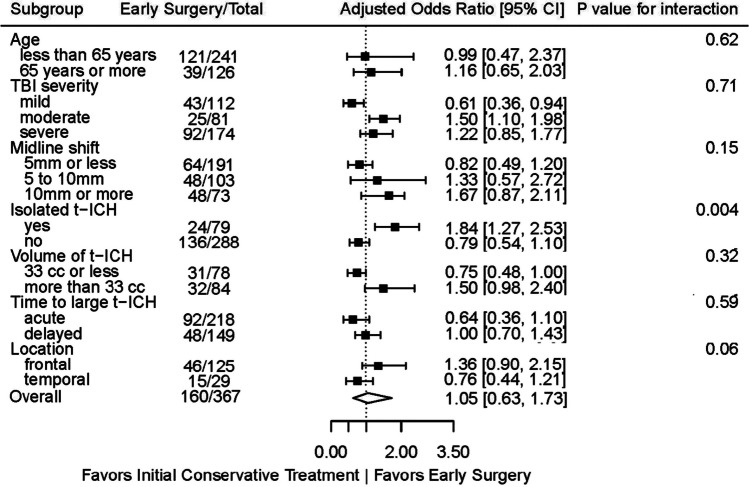
Results: A total of 367 patients with a large t-ICH were included, of whom 160 received early surgery and 207 received conservative treatment. Patients receiving early surgery were younger (median age 54 vs. 58 years) and more severely injured (median Glasgow Coma Scale 7 vs. 10) compared to those treated conservatively. In the overall cohort, early surgery was not associated with better functional outcome (adjusted odds ratio (AOR) 1.1, (95% CI, 0.6-1.7)) compared to conservative treatment. Early surgery was associated with better outcome for patients with moderate TBI and isolated t-ICH (AOR 1.5 (95% CI, 1.1-2.0); P value for interaction 0.71, and AOR 1.8 (95% CI, 1.3-2.5); P value for interaction 0.004). Conversely, in mild TBI and those with a smaller t-ICH (< 33 cc), conservative treatment was associated with better outcome (AOR 0.6 (95% CI, 0.4-0.9); P value for interaction 0.71, and AOR 0.8 (95% CI, 0.5-1.0); P value for interaction 0.32).
Conclusions: Early surgery in t-ICH might benefit those with moderate TBI and isolated t-ICH, comparable with results of the STITCH(Trauma) trial.
Keywords: Conservative treatment; Contusion; Neurosurgery; Surgical treatment; Traumatic intracerebral hematoma.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Bullock MR, et al. Surgical management of traumatic parenchymal lesions. Neurosurgery. 2006;58(3 Suppl):S25–46. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
