

Epidemiological Modeling of the Impact of Public Health Policies on Hepatitis C: Protocol for a Gamification Tool Targeting Microelimination
- PMID: 37747764
- PMCID: PMC10562970
- DOI: 10.2196/38521
Epidemiological Modeling of the Impact of Public Health Policies on Hepatitis C: Protocol for a Gamification Tool Targeting Microelimination
Abstract
Background: Hepatitis C is a disease with a strong social component, as its main transmission route is via blood, making it associated with lifestyle. Therefore, it is suitable to be worked on from the perspective of public health policy, which still has a lot of room to explore and improve, contrary to diagnoses and treatments, which are already very refined and effective.
Objective: An interactive gamified policy tool, designated as Let's End HepC (LEHC), was created to understand the impact of policies related to hepatitis C on the disease's epidemiology on a yearly basis until 2030.
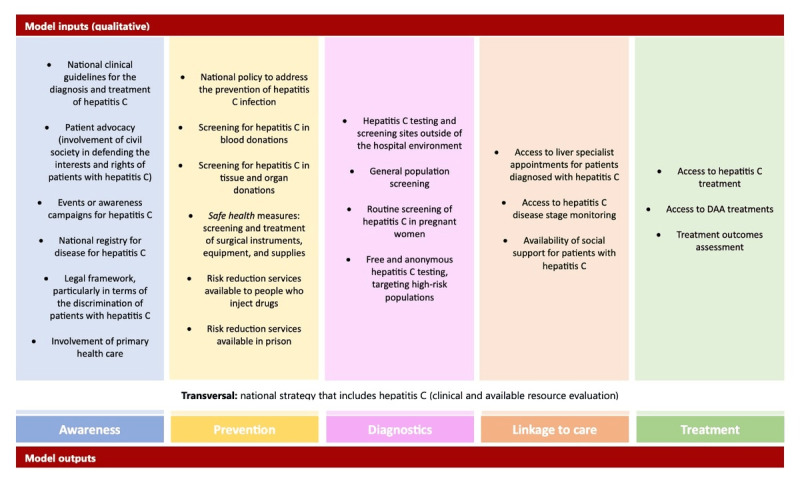
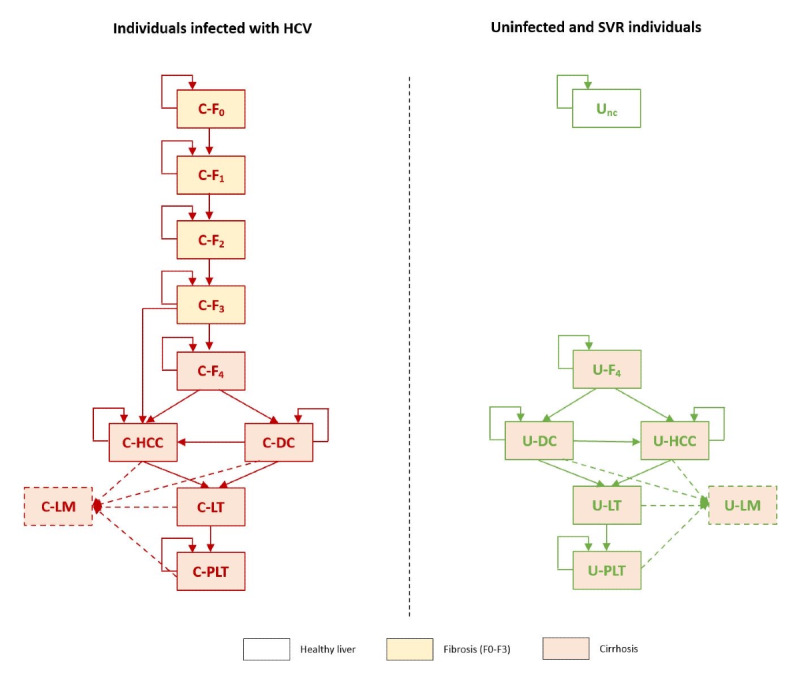
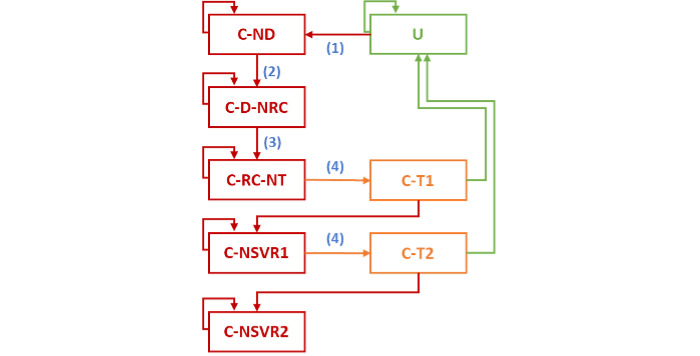
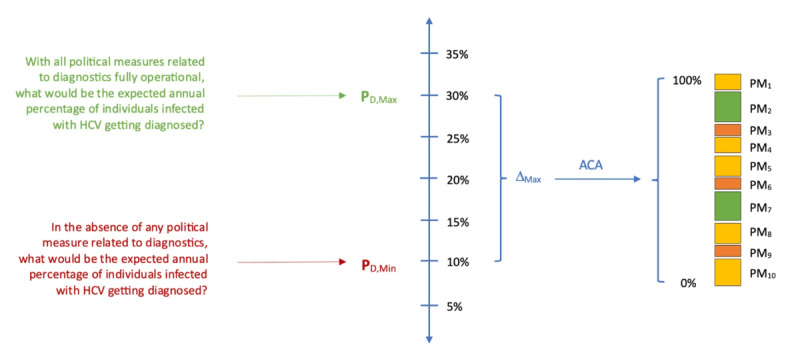
Methods: To this end, an innovative epidemiological model was developed, integrating Markov chains to model the natural history of the disease and adaptive conjoint analysis to reflect the degree of application of each of the 24 public health policies included in the model. This double imputation model makes it possible to assess a set of indicators such as liver transplant, incidence, and deaths year by year until 2030 in different risk groups. Populations at a higher risk were integrated into the model to understand the specific epidemiological dynamics within the total population of each country and within segments that comprise people who have received blood products, prisoners, people who inject drugs, people infected through vertical transmission, and the remaining population.
Results: The model has already been applied to a group of countries, and studies in 5 of these countries have already been concluded, showing results very close to those obtained through other forms of evaluation.
Conclusions: The LEHC model allows the simulation of different degrees of implementation of each policy and thus the verification of its epidemiological impact on each studied population. The gamification feature allows assessing the adequate fulfillment of the World Health Organization goals for the elimination of hepatitis C by 2030. LEHC supports health decision makers and people who practice patient advocacy in making decisions based on science, and because LEHC is democratically shared, it ends up contributing to the increase of citizenship in health.
International registered report identifier (irrid): RR1-10.2196/38521.
Keywords: hepatitis C; mobile phone; modeling; patient advocacy; public health policies.
©Ricardo Baptista-Leite, Henrique Lopes, Björn Vandewalle, Jorge Félix, Diogo Franco, Timo Clemens, Helmut Brand. Originally published in JMIR Research Protocols (https://www.researchprotocols.org), 25.09.2023.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures
Similar articles
-
Let's End HepC: Modelling Public Health Epidemiological Policies Applied to Hepatitis C in Spain.Front Public Health. 2022 Jan 7;9:735572. doi: 10.3389/fpubh.2021.735572. eCollection 2021. Front Public Health. 2022. PMID: 35071151 Free PMC article.
-
Integrating public health policies in the epidemiological modeling of hepatitis C with LEHC tool: application in Austria.Wien Klin Wochenschr. 2021 May;133(9-10):461-469. doi: 10.1007/s00508-020-01774-y. Epub 2020 Dec 17. Wien Klin Wochenschr. 2021. PMID: 33331968 Free PMC article.
-
Modeling the Puzzle of Hepatitis C Epidemiology in Romania: A Pathway to Control.J Gastrointestin Liver Dis. 2020 Sep 9;29(3):377-384. doi: 10.15403/jgld-643. J Gastrointestin Liver Dis. 2020. PMID: 32830821
-
HCV Microelimination for High-risk Special Populations.J Infect Dis. 2023 Sep 13;228(Suppl 3):S168-S179. doi: 10.1093/infdis/jiac446. J Infect Dis. 2023. PMID: 37703340 Review.
-
Hepatitis C Virus Treatment in Children: A Challenge for Hepatitis C Virus Elimination.Semin Liver Dis. 2020 Aug;40(3):213-224. doi: 10.1055/s-0040-1708812. Epub 2020 Jun 11. Semin Liver Dis. 2020. PMID: 32526785 Review.
References
-
- World Health Organization Hepatitis C. World Health Organization. 2022. Jun 24, [2022-12-06]. https://www.who.int/news-room/fact-sheets/detail/hepatitis-c .
-
- Ayoub HH, Chemaitelly H, Omori R, Abu-Raddad LJ. Hepatitis C virus infection spontaneous clearance: has it been underestimated? Int J Infect Dis. 2018 Oct;75:60–6. doi: 10.1016/j.ijid.2018.07.013. https://linkinghub.elsevier.com/retrieve/pii/S1201-9712(18)34472-2 S1201-9712(18)34472-2 - DOI - PubMed
-
- Bulteel N, Partha Sarathy P, Forrest E, Stanley AJ, Innes H, Mills PR, Valerio H, Gunson RN, Aitken C, Morris J, Fox R, Barclay ST. Factors associated with spontaneous clearance of chronic hepatitis C virus infection. J Hepatol. 2016 Aug;65(2):266–72. doi: 10.1016/j.jhep.2016.04.030.S0168-8278(16)30182-9 - DOI - PubMed
LinkOut - more resources
Full Text Sources
