

Impact of Nonselective and Selective α-1 Adrenergic Blockers on the Sedative Efficacy of Dexmedetomidine in Urologic Surgery: A Prospective, Observational Study
- PMID: 37747845
- PMCID: PMC10540644
- DOI: 10.12659/MSM.941614
Impact of Nonselective and Selective α-1 Adrenergic Blockers on the Sedative Efficacy of Dexmedetomidine in Urologic Surgery: A Prospective, Observational Study
Abstract
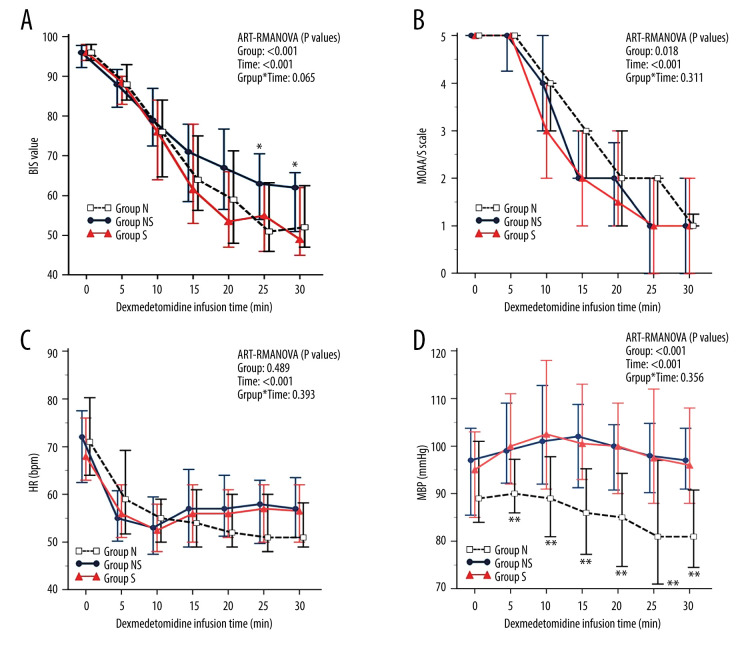
BACKGROUND This study aimed to compare the impact of a-1 adrenergic blockers - nonselective (alfuzosin, doxazosin, and terazosin) and selective (silodosin and tamsulosin) - on the sedative effects of the alpha-2 adrenergic agonist dexmedetomidine (DMT) in patients undergoing urologic surgery. The primary outcome was the sedative effect of DMT as determined by the bispectral index (BIS) and Modified Observer's Assessment of Alertness/Sedation (MOAA/S) scale scores. MATERIAL AND METHODS One hundred eighteen patients undergoing elective urologic surgery with spinal anesthesia were recruited. Patients were assigned based on their medication status to group N (no medication; n=33), group NS (nonselective alpha-1 blocker; n=27), or group S (selective alpha-1 blocker; n=58). Mean blood pressure (MBP), heart rate (HR), oxygen saturation (SpO₂), BIS, and MOAA/S scale scores were recorded at 5-minute (min) intervals after DMT administration. RESULTS Group NS had significantly higher BIS scores than groups N and S at 25 min (P=0.045) and 30 min (P=0.030) after DMT administration, indicating lower sedation levels. MBP significantly differed between the 3 groups at all time points, with group N experiencing a lower MBP than groups NS and S. No significant differences were found between the groups in MOAA/S scale scores, SpO₂, or HR. CONCLUSIONS Nonselective alpha-1 adrenergic blockers can reduce the sedative effects of DMT. Consequently, there may be a need for individualized anesthesia management considering the specific subtype of alpha-1 adrenergic blocker medication.
Conflict of interest statement
Figures
Similar articles
-
Comparison of the performance of phase lag entropy and bispectral index for monitoring the depth of sedation under dexmedetomidine sedation: A prospective, observational, and non-inferiority trial.J Clin Anesth. 2022 Nov;82:110945. doi: 10.1016/j.jclinane.2022.110945. Epub 2022 Aug 25. J Clin Anesth. 2022. PMID: 36029705
-
Adequate sedation with single-dose dexmedetomidine in patients undergoing transurethral resection of the prostate with spinal anaesthesia: a dose-response study by age group.BMC Anesthesiol. 2015 Jan 27;15:17. doi: 10.1186/1471-2253-15-17. BMC Anesthesiol. 2015. PMID: 25971886 Free PMC article. Clinical Trial.
-
A prospective pilotstudy comparing the anesthetic effects of an alpha-2 agonist during holmium laser resection of the prostate and transurethral resection for prostate surgery for benign prostatic hyperplasia patients using selective alpha-1 blockers.BMC Anesthesiol. 2018 Sep 27;18(1):136. doi: 10.1186/s12871-018-0598-1. BMC Anesthesiol. 2018. PMID: 30261833 Free PMC article. Clinical Trial.
-
Target-controlled infusion of dexmedetomidine effect-site concentration for sedation in patients undergoing spinal anaesthesia.J Clin Pharm Ther. 2020 Apr;45(2):347-353. doi: 10.1111/jcpt.13085. Epub 2019 Dec 5. J Clin Pharm Ther. 2020. PMID: 31802541 Clinical Trial.
-
The diagnosis and treatment of lower urinary tract symptoms due to benign prostatic hyperplasia with α-blockers: focus on silodosin.Clin Drug Investig. 2015 Feb;35 Suppl 1:7-18. doi: 10.1007/s40261-014-0257-3. Clin Drug Investig. 2015. PMID: 25708606 Review.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
