

Effect of primaquine dose on the risk of recurrence in patients with uncomplicated Plasmodium vivax: a systematic review and individual patient data meta-analysis
- PMID: 37748496
- PMCID: PMC7615564
- DOI: 10.1016/S1473-3099(23)00430-9
Effect of primaquine dose on the risk of recurrence in patients with uncomplicated Plasmodium vivax: a systematic review and individual patient data meta-analysis
Abstract
Background: Primaquine is used to eliminate Plasmodium vivax hypnozoites, but its optimal dosing regimen remains unclear. We undertook a systematic review and individual patient data meta-analysis to investigate the efficacy and tolerability of different primaquine dosing regimens to prevent P vivax recurrence.
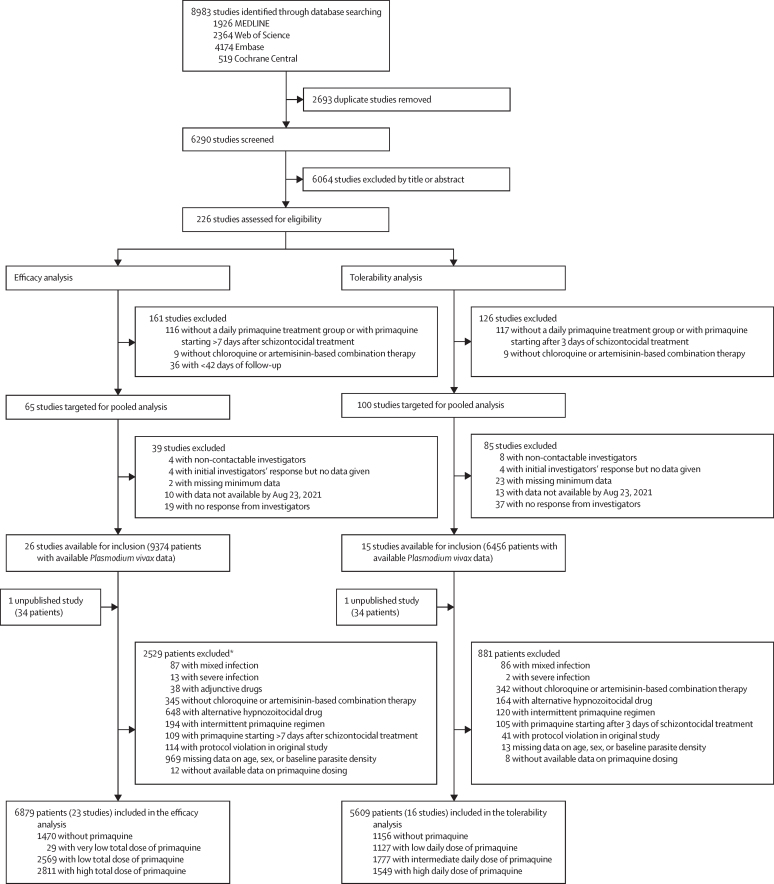
Methods: For this systematic review and individual patient data meta-analysis, we searched MEDLINE, Web of Science, Embase, and Cochrane Central for prospective clinical studies of uncomplicated P vivax from endemic countries published between Jan 1, 2000, and June 8, 2023. We included studies if they had active follow-up of at least 28 days, and if they included a treatment group with daily primaquine given over multiple days, where primaquine was commenced within 7 days of schizontocidal treatment and was given alone or coadministered with chloroquine or one of four artemisinin-based combination therapies (ie, artemether-lumefantrine, artesunate-mefloquine, artesunate-amodiaquine, or dihydroartemisinin-piperaquine). We excluded studies if they were on prevention, prophylaxis, or patients with severe malaria, or if data were extracted retrospectively from medical records outside of a planned trial. For the meta-analysis, we contacted the investigators of eligible trials to request individual patient data and we then pooled data that were made available by Aug 23, 2021. We assessed the effects of total dose and duration of primaquine regimens on the rate of first P vivax recurrence between day 7 and day 180 by Cox's proportional hazards regression (efficacy analysis). The effect of primaquine daily dose on gastrointestinal symptoms on days 5-7 was assessed by modified Poisson regression (tolerability analysis). The study was registered with PROSPERO, CRD42019154470.
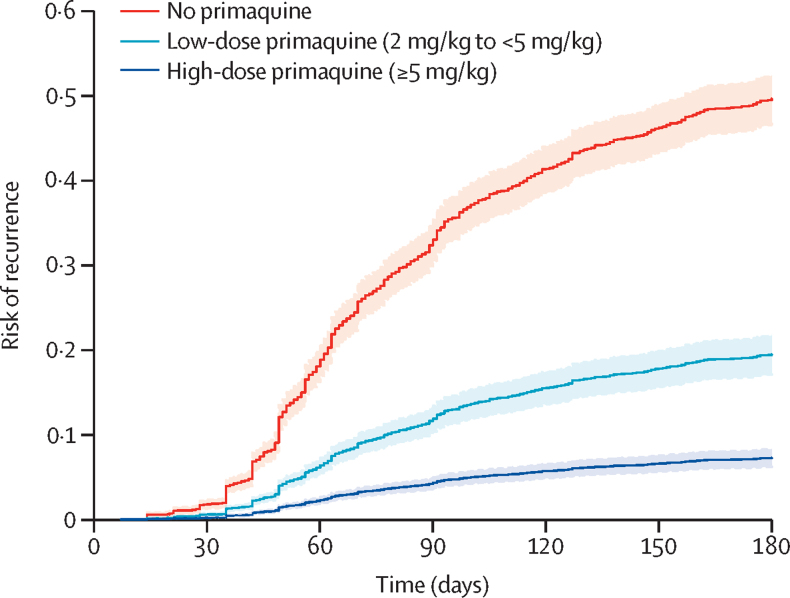
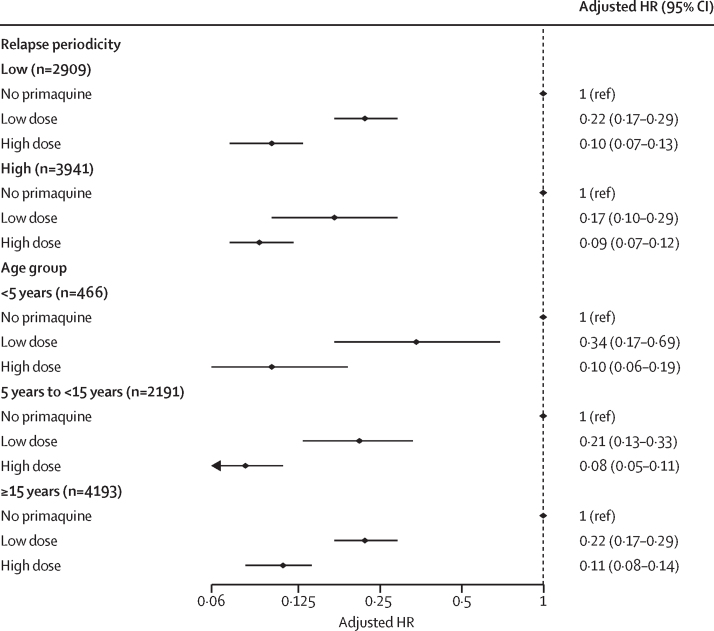
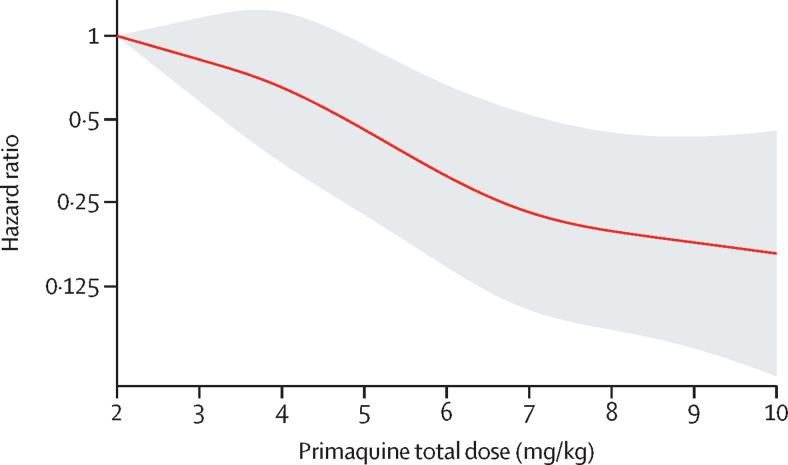
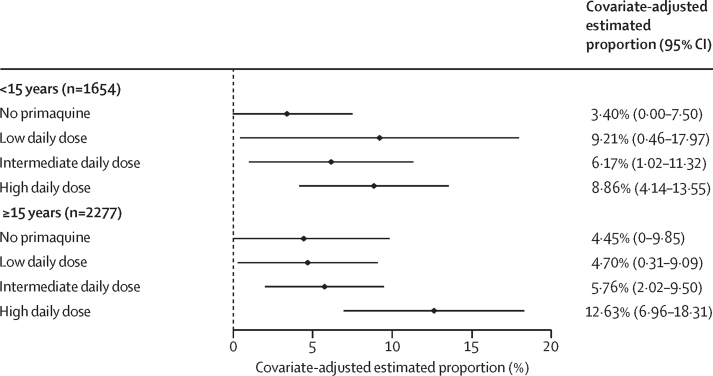
Findings: Of 226 identified studies, 23 studies with patient-level data from 6879 patients from 16 countries were included in the efficacy analysis. At day 180, the risk of recurrence was 51·0% (95% CI 48·2-53·9) in 1470 patients treated without primaquine, 19·3% (16·9-21·9) in 2569 patients treated with a low total dose of primaquine (approximately 3·5 mg/kg), and 8·1% (7·0-9·4) in 2811 patients treated with a high total dose of primaquine (approximately 7 mg/kg), regardless of primaquine treatment duration. Compared with treatment without primaquine, the rate of P vivax recurrence was lower after treatment with low-dose primaquine (adjusted hazard ratio 0·21, 95% CI 0·17-0·27; p<0·0001) and high-dose primaquine (0·10, 0·08-0·12; p<0·0001). High-dose primaquine had greater efficacy than low-dose primaquine in regions with high and low relapse periodicity (ie, the time from initial infection to vivax relapse). 16 studies with patient-level data from 5609 patients from ten countries were included in the tolerability analysis. Gastrointestinal symptoms on days 5-7 were reported by 4·0% (95% CI 0·0-8·7) of 893 patients treated without primaquine, 6·2% (0·5-12·0) of 737 patients treated with a low daily dose of primaquine (approximately 0·25 mg/kg per day), 5·9% (1·8-10·1) of 1123 patients treated with an intermediate daily dose (approximately 0·5 mg/kg per day) and 10·9% (5·7-16·1) of 1178 patients treated with a high daily dose (approximately 1 mg/kg per day). 20 of 23 studies included in the efficacy analysis and 15 of 16 in the tolerability analysis had a low or unclear risk of bias.
Interpretation: Increasing the total dose of primaquine from 3·5 mg/kg to 7 mg/kg can reduce P vivax recurrences by more than 50% in most endemic regions, with a small associated increase in gastrointestinal symptoms.
Funding: Australian National Health and Medical Research Council, Bill & Melinda Gates Foundation, and Medicines for Malaria Venture.
Copyright © 2024 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests JAG and GCKWK are former employees of GSK and hold shares in GSK and AstraZeneca. GCKWK reports travel support from AstraZeneca. JKB reports institutional research funding from Medicines for Malaria Venture, GSK, Wellcome Trust, and Sanaria; participation on the US National Institutes of Health data safety monitoring board; and membership of the editorial board of Travel Medicine and Infectious Disease and the guidelines development group for malaria control and elimination, Global Malaria Programme, WHO. RJC, JKB, and RNP report contributions to Up-to-Date. All other authors declare no competing interests.
Figures
References
-
- WHO . World Health Organization; Geneva: 2022. World malaria report 2022.
-
- WHO . World Health Organization; Geneva: 2022. WHO guidelines for malaria, 25 November 2022.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
