

Reliability and responsiveness of the D12 and validity of its scores as a measure of dyspnoea severity in patients with rheumatoid arthritis-related interstitial lung disease
- PMID: 37748807
- PMCID: PMC10533789
- DOI: 10.1136/bmjresp-2023-001872
Reliability and responsiveness of the D12 and validity of its scores as a measure of dyspnoea severity in patients with rheumatoid arthritis-related interstitial lung disease
Abstract
Background: Interstitial lung disease due to rheumatoid arthritis (RA-ILD) affects a substantial minority of patients with RA, inducing life-altering symptoms, impairing quality of life (QOL) and forcing patients to confront the potential for shortened survival. Dyspnoea is the predominant respiratory symptom of RA-ILD and a strong driver of QOL impairment in patients with it. The D12 is a 12-item questionnaire that assesses the physical and affective components of dyspnoea. It was one of a battery of patient-reported outcomes used in the double-blind, placebo-controlled TRAIL 1 trial of pirfenidone for RA-ILD. There is little information on the reliability, validity or responsiveness of the D12 in RA-ILD.
Methods: In accordance with COSMIN (COnsensus-based Standards for the selection of health Measurement INstruments) methodology, we conducted analyses on data from the TRAIL 1 trial to assess the measurement properties of the D12.
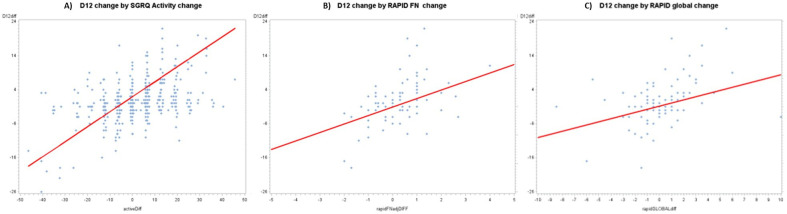
Results: Internal consistency (α=0.95, 0.95, 0.95, 0.95 and 0.96 at baseline, 13, 26, 39 and 52 weeks) and test-retest reliability 0.85 (0.71 to 0.92) exceeded acceptability criteria. Well over the 75% benchmark of hypotheses (43/46=93%) around D12 measurement properties were confirmed. Known-groups validity was supported by significant differences between subgroups of patients with differing levels of dyspnoea (eg, St. George's Respiratory Questionnaire (SGRQ) Activity score ≥50 vs <50, 9.36 (1.27) points, p<0.0001, with a large effect size=1.7) and physiological impairment at baseline. Longitudinal validity was supported by significant associations between D12 and anchor scores over time (eg, at 52 weeks, correlation between D12 change and SGRQ Activity change was 0.54, p<0.0001; between D12 change and Routine Assessment of Patient Index Data (RAPID) Functioning Component was 0.41, p<0.0001). A battery of analyses confirmed the responsiveness of D12 scores for capturing change in dyspnoea over time. We estimated the minimal within-patient change threshold for worsening as 3 points.
Conclusions: D12 scores possess acceptable measurement properties in RA-ILD, such that it can be used with confidence in this population to assess dyspnoea severity defined by its physical and affective components. As validation is an ongoing process, and never accomplished in a single study, additional research on the psychometric properties of the D12 in RA-ILD is encouraged.
Keywords: interstitial fibrosis; surveys and questionnaires; systemic disease and lungs.
© Author(s) (or their employer(s)) 2023. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
Similar articles
-
Reliability, validity and responsiveness to change of the Saint George's Respiratory Questionnaire in early diffuse cutaneous systemic sclerosis.Rheumatology (Oxford). 2015 Aug;54(8):1369-79. doi: 10.1093/rheumatology/keu456. Epub 2015 Feb 9. Rheumatology (Oxford). 2015. PMID: 25667436 Free PMC article.
-
Evaluation of rheumatoid arthritis and connective tissue disease-related interstitial lung disease with pulmonary physiologic test, HRCT, and patient-based measures of dyspnea and functional disability.Clin Rheumatol. 2021 Sep;40(9):3797-3805. doi: 10.1007/s10067-021-05693-9. Epub 2021 Apr 3. Clin Rheumatol. 2021. PMID: 33811590
-
Survival and quality of life in rheumatoid arthritis-associated interstitial lung disease after lung transplantation.J Heart Lung Transplant. 2014 May;33(5):514-20. doi: 10.1016/j.healun.2014.01.858. Epub 2014 Jan 24. J Heart Lung Transplant. 2014. PMID: 24630861
-
Recent advances in rheumatoid arthritis-associated interstitial lung disease.Curr Opin Pulm Med. 2020 Sep;26(5):477-486. doi: 10.1097/MCP.0000000000000710. Curr Opin Pulm Med. 2020. PMID: 32701675 Review.
-
Rheumatoid arthritis-associated interstitial lung disease: an overview of epidemiology, pathogenesis and management.Clin Rheumatol. 2021 Apr;40(4):1211-1220. doi: 10.1007/s10067-020-05320-z. Epub 2020 Aug 13. Clin Rheumatol. 2021. PMID: 32794076 Review.
Cited by
-
Validation of "Clinical Red Flags" for RA-ILD in an Italian cohort.Front Med (Lausanne). 2025 Jul 16;12:1625742. doi: 10.3389/fmed.2025.1625742. eCollection 2025. Front Med (Lausanne). 2025. PMID: 40740947 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials