

Regional variations in short stay urgent paediatric hospital admissions: a sequential mixed-methods approach exploring differences through data linkage and qualitative interviews
- PMID: 37748848
- PMCID: PMC10533722
- DOI: 10.1136/bmjopen-2023-072734
Regional variations in short stay urgent paediatric hospital admissions: a sequential mixed-methods approach exploring differences through data linkage and qualitative interviews
Abstract
Objectives: The aim of this sequential mixed-methods study was to describe and understand how paediatric short stay admission (SSA) rates vary across Health Board regions of Scotland.
Design: Exploratory sequential mixed-methods study. Routinely acquired data for the annual (per capita) SSA to hospital were compared across the 11 regions. Five diverse regions with different SSA per capita formed cases for qualitative interviews with health professionals and parents to explore how care pathways, service features and geography may influence decisions to admit.
Setting: Scotland.
Participants: All children admitted to hospital 2015-2017. Healthcare staff (n=48) and parents (n=15) were interviewed.
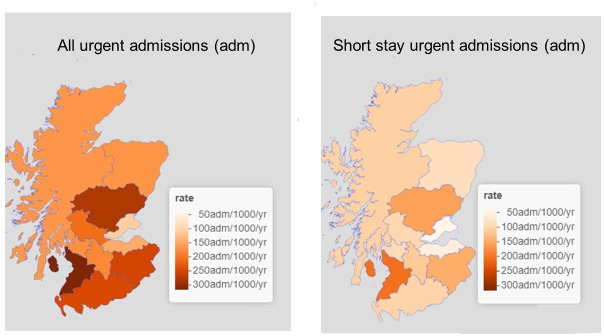
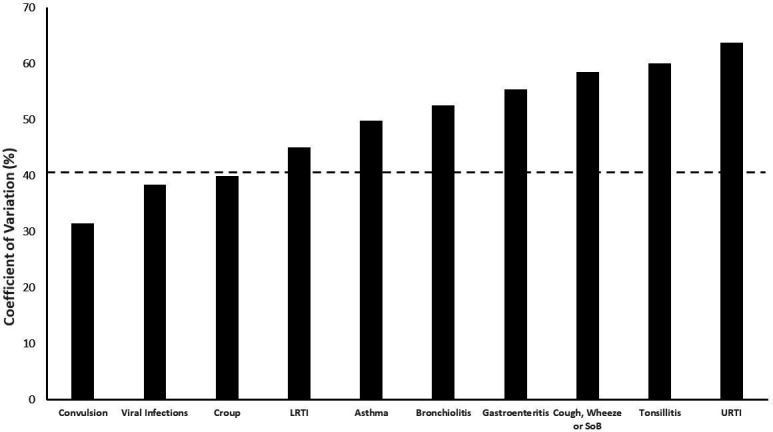
Results: Of 171 039 urgent hospital admissions, 92 229 were SSAs, with a fivefold variation between 14 and 69/1000 children/year across regions. SSAs were higher for children in the most deprived compared with the least deprived communities. When expressed as a ratio of highest to lowest SSA/1000 children/year for diagnosed conditions between regions, the ratio was highest (10.1) for upper respiratory tract infection and lowest (2.8) for convulsions. Readmissions varied between 0.80 and 2.52/1000/year, with regions reporting higher SSA rates more likely to report higher readmission rates (r=0.70, p=0.016, n=11). Proximity and ease of access to services, local differences in service structure and configuration, national policy directives and disparities in how an SSA is defined were recognised by interviewees as explaining the observed regional variations in SSAs. Socioeconomic deprivation was seldom spontaneously raised by professionals when reflecting on reasons to refer or admit a child. Instead, greater emphasis was placed on the wider social circumstances and parents' capacity to cope with and manage their child's illness at home.
Conclusion: SSA rates for children vary quantitatively by region, condition and area deprivation and our interviews identify reasons for this. These findings can usefully inform future care pathway interventions.
Keywords: health services accessibility; organisation of health services; paediatric A&E and ambulatory care.
© Author(s) (or their employer(s)) 2023. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
Similar articles
-
Identifying and prioritising future interventions with stakeholders to improve paediatric urgent care pathways in Scotland, UK: a mixed-methods study.BMJ Open. 2023 Oct 12;13(10):e074141. doi: 10.1136/bmjopen-2023-074141. BMJ Open. 2023. PMID: 37827745 Free PMC article.
-
Short-stay urgent hospital admissions of children with convulsions: A mixed methods exploratory study to inform out of hospital care pathways.PLoS One. 2024 Apr 1;19(4):e0301071. doi: 10.1371/journal.pone.0301071. eCollection 2024. PLoS One. 2024. PMID: 38557817 Free PMC article.
-
Short stay hospital admissions for an acutely unwell child: A qualitative study of outcomes that matter to parents and professionals.PLoS One. 2022 Dec 16;17(12):e0278777. doi: 10.1371/journal.pone.0278777. eCollection 2022. PLoS One. 2022. PMID: 36525432 Free PMC article.
-
Identifying models of care to improve outcomes for older people with urgent care needs: a mixed methods approach to develop a system dynamics model.Health Soc Care Deliv Res. 2023 Sep;11(14):1-183. doi: 10.3310/NLCT5104. Health Soc Care Deliv Res. 2023. PMID: 37830206 Review.
-
Explaining variation in emergency admissions: a mixed-methods study of emergency and urgent care systems.Southampton (UK): NIHR Journals Library; 2014 Dec. Southampton (UK): NIHR Journals Library; 2014 Dec. PMID: 25642501 Free Books & Documents. Review.
Cited by
-
Identifying and prioritising future interventions with stakeholders to improve paediatric urgent care pathways in Scotland, UK: a mixed-methods study.BMJ Open. 2023 Oct 12;13(10):e074141. doi: 10.1136/bmjopen-2023-074141. BMJ Open. 2023. PMID: 37827745 Free PMC article.
-
Short-stay urgent hospital admissions of children with convulsions: A mixed methods exploratory study to inform out of hospital care pathways.PLoS One. 2024 Apr 1;19(4):e0301071. doi: 10.1371/journal.pone.0301071. eCollection 2024. PLoS One. 2024. PMID: 38557817 Free PMC article.
-
Rising Unscheduled Healthcare Utilisation of Children and Young People: How Does the Rise Vary Across Deprivation Quintiles in UK Nations?Health Serv Insights. 2024 May 29;17:11786329241245235. doi: 10.1177/11786329241245235. eCollection 2024. Health Serv Insights. 2024. PMID: 38817927 Free PMC article.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials