

Clinical Features and Neurotologic Findings in Patients With Acute Unilateral Peripheral Vestibulopathy Associated With Antiganglioside Antibody
- PMID: 37748887
- PMCID: PMC10663017
- DOI: 10.1212/WNL.0000000000207814
Clinical Features and Neurotologic Findings in Patients With Acute Unilateral Peripheral Vestibulopathy Associated With Antiganglioside Antibody
Abstract
Background and objectives: Anecdotal studies have reported the presence of antiganglioside antibodies in acute unilateral peripheral vestibulopathy (AUPV). This study aimed to determine the prevalence, clinical characteristics, and neurotologic findings of AUPV associated with antiganglioside antibodies.
Methods: Serum antigangliosides were measured in consecutive patients with AUPV according to the Bárány Society criteria during the acute and recovery phases in a referral-based university hospital in South Korea from September 2019 to January 2023. Clinical characteristics and neurotologic findings were compared between those with and without antiganglioside antibodies. The results of video-oculography, video head impulse and bithermal caloric tests, and other neurotologic evaluations including ocular and cervical vestibular-evoked myogenic potentials and subjective visual vertical were compared between the 2. MRIs dedicated to the inner ear were also conducted when considered necessary.
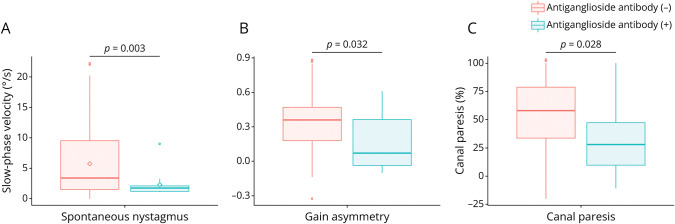
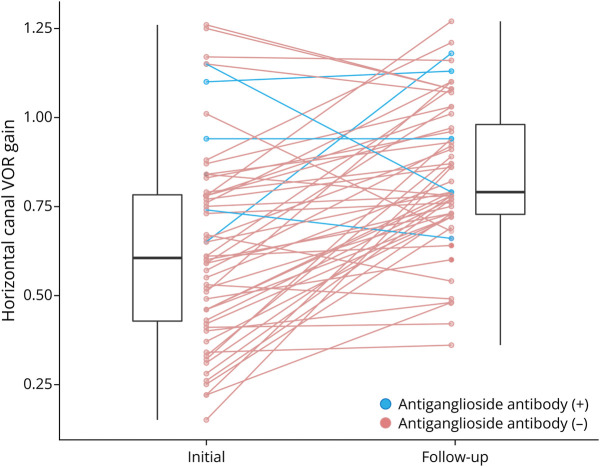
Results: One hundred five patients (mean age ± SD = 60 ± 13 years, 57 male) were included for analyses. During the acute phase, 12 patients (12/105, 11%) were tested positive for serum antiganglioside antibodies, including anti-GQ1b immunoglobulin (Ig) G (n = 5) or IgM (n = 4), anti-GM1 IgM (n = 3), and anti-GD1a IgG (n = 1, including 1 patient with a positive anti-GQ1b antibody). Patients with antiganglioside antibodies showed lesser intensity of spontaneous nystagmus (median [interquartile range] = 1.8 [1.2-2.1] vs 3.4 [1.5-9.5], p = 0.003) and a lesser degree of canal paresis (30 [17-47] vs 58 [34-79], p = 0.028) and gain asymmetry of the vestibulo-ocular reflex for the horizontal semicircular canal during head impulse tests (0.07 [-0.04 to 0.61] vs 0.36 [0.18-0.47], p = 0.032) than those without antibodies. Negative conversion of antibodies and vestibular recovery were observed in most patients (6/8, 75%). Among 30 patients with AUPV with 4-hour delayed 3D fluid-attenuated inversion recovery dedicated to the inner ear, gadolinium enhancement was observed in 18 (18/30, 60%), either in the vestibule (n = 9), semicircular canal (n = 6), or vestibular nerve (n = 5). The positivity rates based on specific antibodies could not be determined due to limited sample sizes.
Discussion: The association between antiganglioside antibodies and AUPV suggests an immune-mediated mechanism in acute vestibular failure and extends the clinical spectrum of antiganglioside antibody syndrome.
© 2023 American Academy of Neurology.
Conflict of interest statement
K.T. Kim, E. Park, S.-U. Lee, and B. Kim report no relevant disclosures. B.J. Kim serves as an Editor-in-Chief of the
Figures
Similar articles
-
Four-hour-delayed 3D-FLAIR MRIs in patients with acute unilateral peripheral vestibulopathy.Ann Clin Transl Neurol. 2024 Aug;11(8):2030-2039. doi: 10.1002/acn3.52123. Epub 2024 Jun 14. Ann Clin Transl Neurol. 2024. PMID: 38874375 Free PMC article.
-
Selective otolithic dysfunction in patients presenting with acute spontaneous vertigo: consideration based on MRI.Front Neurol. 2024 Dec 23;15:1517112. doi: 10.3389/fneur.2024.1517112. eCollection 2024. Front Neurol. 2024. PMID: 39777315 Free PMC article.
-
Visuospatial cognition in acute unilateral peripheral vestibulopathy.Front Neurol. 2023 Sep 14;14:1230495. doi: 10.3389/fneur.2023.1230495. eCollection 2023. Front Neurol. 2023. PMID: 37789890 Free PMC article.
-
Isolated vestibular nuclear infarction: report of two cases and review of the literature.J Neurol. 2014 Jan;261(1):121-9. doi: 10.1007/s00415-013-7139-0. Epub 2013 Oct 27. J Neurol. 2014. PMID: 24162036 Review.
-
Acute vestibular syndrome associated with anti-GQ1b antibody.Neurology. 2019 Sep 10;93(11):e1085-e1092. doi: 10.1212/WNL.0000000000008107. Epub 2019 Aug 9. Neurology. 2019. PMID: 31399495
Cited by
-
Four-hour-delayed 3D-FLAIR MRIs in patients with acute unilateral peripheral vestibulopathy.Ann Clin Transl Neurol. 2024 Aug;11(8):2030-2039. doi: 10.1002/acn3.52123. Epub 2024 Jun 14. Ann Clin Transl Neurol. 2024. PMID: 38874375 Free PMC article.
-
Bilaterally positive head-impulse tests can differentiate AICA infarction from labyrinthitis.Front Neurol. 2024 Aug 29;15:1448989. doi: 10.3389/fneur.2024.1448989. eCollection 2024. Front Neurol. 2024. PMID: 39268064 Free PMC article.
-
Latent antiganglioside antibodies-related ophthalmoplegia revealed by head impulse test: a new role for an old sign.J Neurol. 2025 Feb 11;272(3):187. doi: 10.1007/s00415-025-12946-z. J Neurol. 2025. PMID: 39932598 No abstract available.
-
Selective otolithic dysfunction in patients presenting with acute spontaneous vertigo: consideration based on MRI.Front Neurol. 2024 Dec 23;15:1517112. doi: 10.3389/fneur.2024.1517112. eCollection 2024. Front Neurol. 2024. PMID: 39777315 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources