

Rapid emergence and transmission of virulence-associated mutations in the oral poliovirus vaccine following vaccination campaigns
- PMID: 37749086
- PMCID: PMC10520055
- DOI: 10.1038/s41541-023-00740-9
Rapid emergence and transmission of virulence-associated mutations in the oral poliovirus vaccine following vaccination campaigns
Abstract
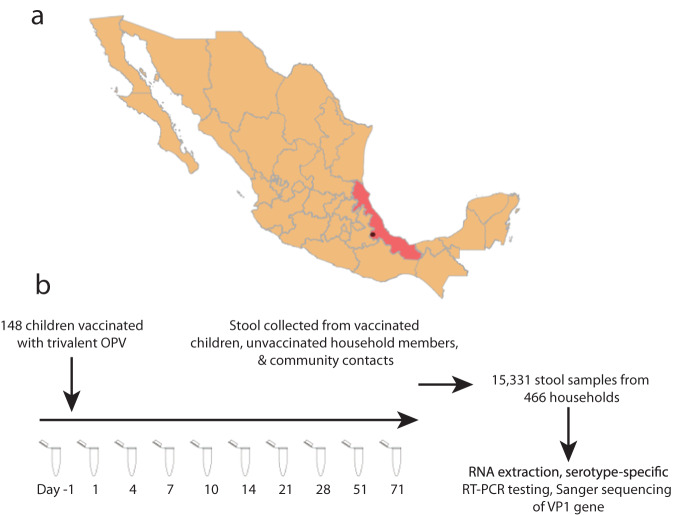
There is an increasing burden of circulating vaccine-derived polioviruses (cVDPVs) due to the continued use of oral poliovirus vaccine (OPV). However, the informativeness of routine OPV VP1 sequencing for the early identification of viruses carrying virulence-associated reversion mutations has not been directly evaluated in a controlled setting. We prospectively collected 15,331 stool samples to track OPV shedding from children receiving OPV and their contacts for ten weeks following an immunization campaign in Veracruz State, Mexico and sequenced VP1 genes from 358 samples. We found that OPV was genetically unstable and evolves at an approximately clocklike rate that varies across serotypes and by vaccination status. Overall, 61% (11/18) of OPV-1, 71% (34/48) OPV-2, and 96% (54/56) OPV-3 samples with available data had evidence of a reversion at the key 5' UTR attenuating position and 28% (13/47) of OPV-1, 12% (14/117) OPV-2, and 91% (157/173) OPV-3 of Sabin-like viruses had ≥1 known reversion mutations in the VP1 gene. Our results are consistent with previous work documenting rapid reversion to virulence of OPV and underscores the need for intensive surveillance following OPV use.
© 2023. Springer Nature Limited.
Conflict of interest statement
The authors declare no competing interests.
Figures




Update of
-
Rapid emergence and transmission of virulence-associated mutations in the oral poliovirus vaccine following vaccination campaigns.medRxiv [Preprint]. 2023 Mar 21:2023.03.16.23287381. doi: 10.1101/2023.03.16.23287381. medRxiv. 2023. Update in: NPJ Vaccines. 2023 Sep 25;8(1):137. doi: 10.1038/s41541-023-00740-9. PMID: 36993386 Free PMC article. Updated. Preprint.
References
-
- Macklin, G. R. et al. Epidemiology of type 2 vaccine-derived poliovirus outbreaks between 2016 and 2020. Vaccine (2022) 10.1016/j.vaccine.2022.08.008. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
