

FGF-23 is a biomarker of RV dysfunction and congestion in patients with HFrEF
- PMID: 37749114
- PMCID: PMC10520041
- DOI: 10.1038/s41598-023-42558-4
FGF-23 is a biomarker of RV dysfunction and congestion in patients with HFrEF
Abstract
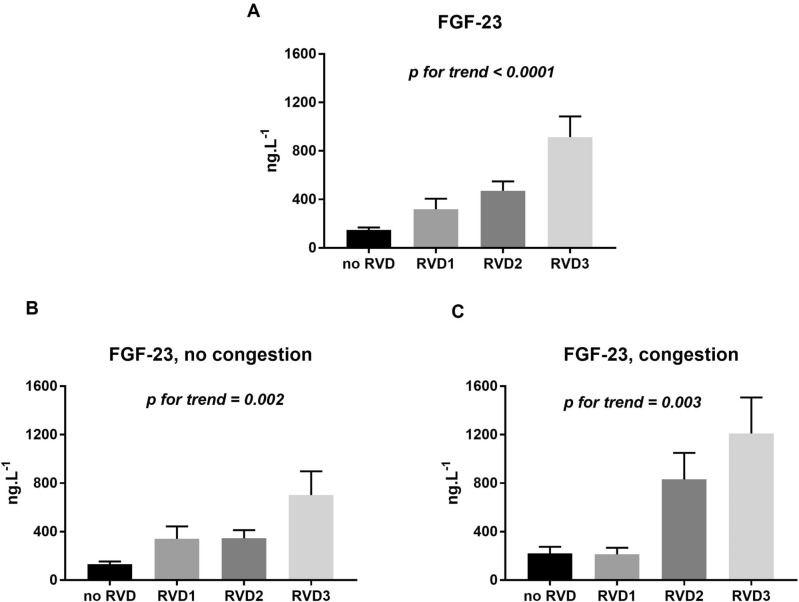
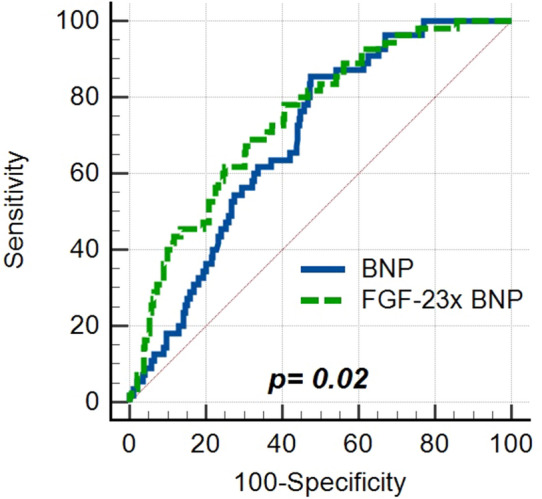
There is no biomarker reflecting right ventricular dysfunction in HFrEF patients used in clinical practice. We have aimed to look for a circulating marker of RV dysfunction employing a quantitative proteomic strategy. The Olink Proteomics Multiplex panels (Cardiovascular Disease II, III, Cardiometabolic, and Inflammation Target Panels) identified FGF-23 to be the most differentially abundant (more than 2.5-fold) in blood plasma of HF patients with severe RV dysfunction (n = 30) compared to those with preserved RV function (n = 31). A subsequent ELISA-based confirmatory analysis of circulating FGF-23 in a large cohort of patients (n = 344, 72.7% NYHA III/IV, LVEF 22.5%, 54.1% with moderate/severe RV dysfunction), followed by multivariable regression analysis, revealed that the plasma FGF-23 level was most significantly associated with RV dysfunction grade (p = 0.0004) and congestion in the systemic circulation (p = 0.03), but not with LV-ejection fraction (p = 0.69) or estimated glomerular filtration rate (eGFR, p = 0.08). FGF-23 was associated with the degree of RV dysfunction in both sub-cohorts (i.e. in patients with and without congestion, p < 0.0001). The association between FGF-23 and RV-dysfunction remained significant after the adjustment for BNP (p = 0.01). In contrast, when adjusted for BNP, FGF-23 was no longer associated with LV dysfunction (p = 0.59). The Cox proportional hazard model revealed that circulating FGF-23 was significantly associated with adverse outcomes even after adjusting for BNP, LVEF, RV dysfunction grade and eGFR. Circulating FGF-23 is thus a biomarker of right ventricular dysfunction in HFrEF patients regardless of congestion status.
© 2023. Springer Nature Limited.
Conflict of interest statement
Josef Kautzner is a member of Advisory Boards for Boehringer Ingelheim, Biosense Webster, Medtronic and St Jude Medical (Abbott). He has received speaker honoraria from the above-mentioned companies and from Biotronik, Cath Vision, Pfizer and Pro Med CS. Petr Jarolim received research support from Abbott Laboratories, Amgen, Inc., AstraZeneca, LP, Daiichi-Sankyo, Inc., GlaxoSmithKline, Merck & Co., Inc., Regeneron, Roche Diagnostics Corporation, and Siemens Healthineers. Remaining authors do not possess Competing Interest.
Figures

References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
