

Intrathecal dexmedetomidine as an adjuvant to plain ropivacaine for spinal anesthesia during cesarean section: a prospective, double-blinded, randomized trial for ED50 determination using an up-down sequential allocation method
- PMID: 37749533
- PMCID: PMC10519004
- DOI: 10.1186/s12871-023-02275-x
Intrathecal dexmedetomidine as an adjuvant to plain ropivacaine for spinal anesthesia during cesarean section: a prospective, double-blinded, randomized trial for ED50 determination using an up-down sequential allocation method
Abstract
Background: Intrathecal dexmedetomidine, as an adjuvant to local anesthetics, has been reported to improve the quality of spinal anesthesia and reduce the required local anesthetic dose. However, the optimal dosage regimen for intrathecal dexmedetomidine combined with plain ropivacaine for cesarean section (CS) remains undetermined. The present study aimed to determine the median effective dose (ED50) of intrathecal dexmedetomidine as an adjuvant to plain ropivacaine for spinal anesthesia during CS.
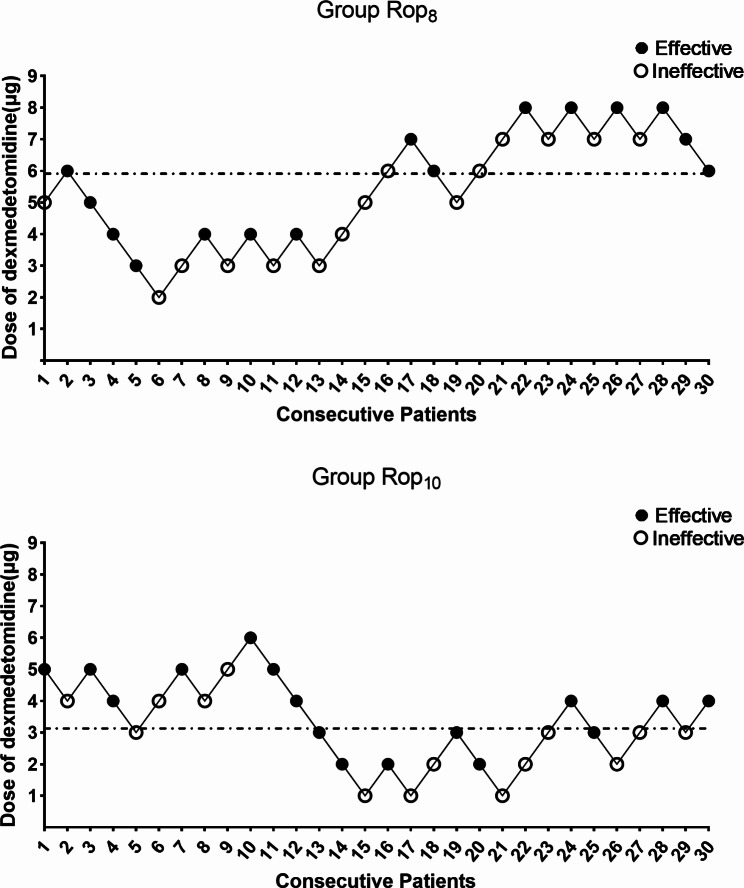
Methods: Sixty parturients undergoing CS were randomly assigned to either group: plain ropivacaine 8 mg (Group Rop8) or plain ropivacaine 10 mg (Group Rop10). The initial dosage of intrathecal dexmedetomidine in each group was 5 µg. The effective dose was defined as a bilateral sensory block at the level of T6 or above to pinprick attained within 10 min after intrathecal injection, without the need for supplementary intraoperative epidural anesthesia. Effective or ineffective responses were determined, followed by a 1 µg increment or decrement in the dose of intrathecal dexmedetomidine for the next parturient using up-down sequential allocation. ED50 were calculated using probit regression.
Results: The ED50 of intrathecal dexmedetomidine with plain ropivacaine was 5.9 µg (95% confidence interval [CI], 4.9-7.4 µg) in Group Rop8 and 3.1 µg (95% CI, 0.1-4.8 µg) in Group Rop10 (P < 0.05). Hemodynamic stability, side effects, patient satisfaction and neonatal outcomes were comparable between the two groups.
Conclusions: The present data suggested that the ED50 of intrathecal dexmedetomidine as an adjuvant to 8 mg and 10 mg plain ropivacaine in spinal anesthesia during cesarean section was approximately 6 µg and 3 µg, respectively.
Trial registration: Chinese Clinical Trial Registry, identifier: ChiCTR2200055928.
Keywords: Cesarean section; Dexmedetomidine; Ropivacaine; Spinal anesthesia.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
The authors declare that there are no competing interests associated with the manuscript.
Figures


References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
