

Development and validation of a clinical prediction model for detecting coronary heart disease in middle-aged and elderly people: a diagnostic study
- PMID: 37749613
- PMCID: PMC10521501
- DOI: 10.1186/s40001-023-01233-0
Development and validation of a clinical prediction model for detecting coronary heart disease in middle-aged and elderly people: a diagnostic study
Abstract
Objective: To develop and validate a multivariate prediction model to estimate the risk of coronary heart disease (CHD) in middle-aged and elderly people and to provide a feasible method for early screening and diagnosis in middle-aged and elderly CHD patients.
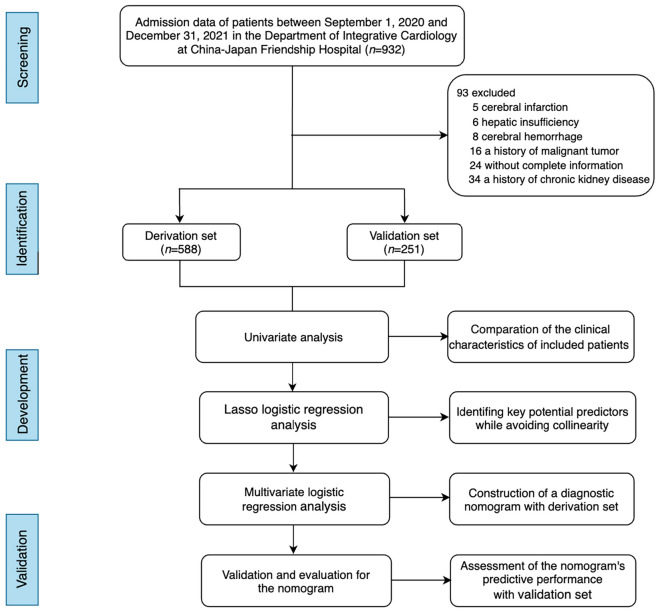
Methods: This study was a single-center, retrospective, case-control study. Admission data of 932 consecutive patients with suspected CHD were retrospectively assessed from September 1, 2020 to December 31, 2021 in the Department of Integrative Cardiology at China-Japan Friendship Hospital. A total of 839 eligible patients were included in this study, and 588 patients were assigned to the derivation set and 251 as the validation set at a 7:3 ratio. Clinical characteristics of included patients were compared between derivation set and validation set by univariate analysis. The least absolute shrinkage and selection operator (Lasso) regression analysis method was performed to avoid collinearity and identify key potential predictors. Multivariate logistic regression analysis was used to construct a clinical prediction model with identified predictors for clinical practice. Bootstrap validation was used to test performance and eventually we obtained the actual model. And the Hosmer-Lemeshow test was carried out to evaluate the goodness-fit of the constructed model. The area under curve (AUC) of receiver operating characteristic (ROC), calibration curve, decision curve analysis (DCA), and clinical impact curve (CIC) were plotted and utilized with validation set to comprehensively evaluate the predictive accuracy and clinical value of the model.
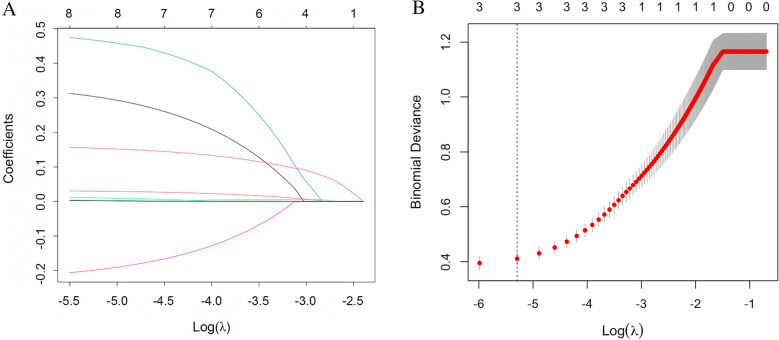
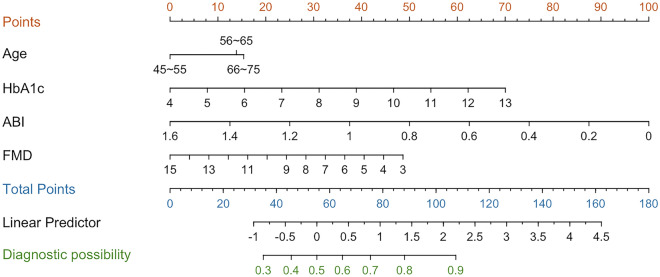
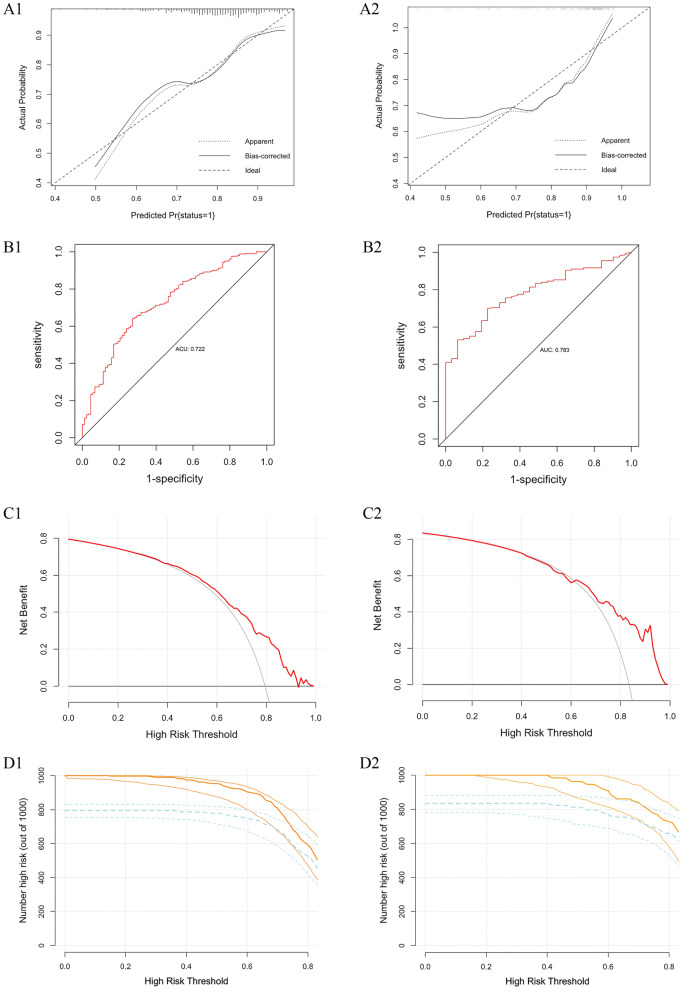
Results: A total of eight indicators were identified as risk factors for the development of CHD in middle-aged and elderly people by univariate analysis. Of these candidate predictors, four key parameters were defined to be significantly related to CHD by Lasso regression analysis, including age (OR 1.034, 95% CI 1.002 ~ 1.067, P = 0.040), hemoglobin A1c (OR 1.380, 95% CI 1.078 ~ 1.768, P = 0.011), ankle-brachial index (OR 0.078, 95% CI 0.012 ~ 0.522, P = 0.009), and brachial artery flow-mediated vasodilatation (OR 0.848, 95% CI 0.726 ~ 0.990, P = 0.037). The Hosmer-Lemeshow test showed a good calibration performance of the clinical prediction model (derivation set, χ2 = 7.865, P = 0.447; validation set, χ2 = 11.132, P = 0.194). The ROCs of the nomogram in the derivation set and validation set were 0.722 and 0.783, respectively, suggesting excellent predictive power and suitable performance. The clinical prediction model presented a greater net benefit and clinical impact based on DCA and CIC analysis.
Conclusion: Overall, the development and validation of the multivariate model combined the laboratory and clinical parameters of patients with CHD, which could be beneficial to the individualized prediction of middle-aged and elderly people, and helped to facilitate clinical assessments and decisions during treatment and management of CHD.
Keywords: Clinical prediction model; Coronary heart disease; Diagnostic study; Nomogram; Risk factor.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Development, assessment and validation of a novel nomogram model for predicting stroke mimics in stroke center:A single-center observational study.Heliyon. 2024 Sep 27;10(19):e38602. doi: 10.1016/j.heliyon.2024.e38602. eCollection 2024 Oct 15. Heliyon. 2024. PMID: 39403531 Free PMC article.
-
[Construction and validation of a nomogram for predicting in-hospital postoperative heart failure in elderly patients with hip fracture].Beijing Da Xue Xue Bao Yi Xue Ban. 2024 Oct 18;56(5):874-883. doi: 10.19723/j.issn.1671-167X.2024.05.019. Beijing Da Xue Xue Bao Yi Xue Ban. 2024. PMID: 39397468 Free PMC article. Chinese.
-
Establishment and Validation of a Non-invasive Diagnostic Nomogram to Identify Heart Failure in Patients With Coronary Heart Disease.Front Cardiovasc Med. 2022 Apr 7;9:875702. doi: 10.3389/fcvm.2022.875702. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 35463796 Free PMC article.
-
Development and validation of frailty risk prediction model for elderly patients with coronary heart disease.BMC Geriatr. 2024 Sep 7;24(1):742. doi: 10.1186/s12877-024-05320-7. BMC Geriatr. 2024. PMID: 39244543 Free PMC article.
-
Research inefficiencies in external validation studies of the Framingham Wilson coronary heart disease risk rule: A systematic review.PLoS One. 2024 Sep 13;19(9):e0310321. doi: 10.1371/journal.pone.0310321. eCollection 2024. PLoS One. 2024. PMID: 39269949 Free PMC article.
Cited by
-
Construction and validation of a readmission risk prediction model for elderly patients with coronary heart disease.Front Cardiovasc Med. 2024 Dec 18;11:1497916. doi: 10.3389/fcvm.2024.1497916. eCollection 2024. Front Cardiovasc Med. 2024. PMID: 39744210 Free PMC article.
-
Feasibility of tongue image detection for coronary artery disease: based on deep learning.Front Cardiovasc Med. 2024 Aug 23;11:1384977. doi: 10.3389/fcvm.2024.1384977. eCollection 2024. Front Cardiovasc Med. 2024. PMID: 39246581 Free PMC article.
-
Progress Analysis of Personalized Antiplatelet Therapy in Patients with Coronary Heart Disease Undergoing Interventional Therapy.Rev Cardiovasc Med. 2024 Dec 25;25(12):462. doi: 10.31083/j.rcm2512462. eCollection 2024 Dec. Rev Cardiovasc Med. 2024. PMID: 39742248 Free PMC article. Review.
References
-
- Roth GA, Mensah GA, Johnson CO, Addolorato G, Ammirati E, Baddour LM, et al. GBD-NHLBI-JACC global burden of cardiovascular diseases writing group. global burden of cardiovascular diseases and risk factors, 1990–2019 update from the GBD 2019 study. J Am Coll Cardiol. 2020;76:2982–3021. doi: 10.1016/j.jacc.2020.11.010. - DOI - PMC - PubMed
-
- Nowbar AN, Howard JP, Finegold JA, Asaria P, Francis DP. 2014 global geographic analysis of mortality from ischaemic heart disease by country, age and income: statistics from World Health Organisation and United Nations. Int J Cardiol. 2014;174:293–298. doi: 10.1016/j.ijcard.2014.04.096. - DOI - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
