

Comparative Efficacy, Durability and Safety of Faricimab in the Treatment of Diabetic Macular Edema: A Systematic Literature Review and Network Meta-Analysis
- PMID: 37751021
- PMCID: PMC10937806
- DOI: 10.1007/s12325-023-02675-y
Comparative Efficacy, Durability and Safety of Faricimab in the Treatment of Diabetic Macular Edema: A Systematic Literature Review and Network Meta-Analysis
Erratum in
-
Correction to: Comparative Efficacy, Durability and Safety of Faricimab in the Treatment of Diabetic Macular Edema: A Systematic Literature Review and Network Meta-Analysis.Adv Ther. 2024 May;41(5):2084-2085. doi: 10.1007/s12325-024-02831-y. Adv Ther. 2024. PMID: 38480662 Free PMC article. No abstract available.
Abstract
Introduction: A systematic literature review (SLR) and network meta-analysis (NMA) were conducted to evaluate the comparative efficacy, durability and safety of faricimab, used in a Treat & Extend (T&E) regime with intervals up to every 16 weeks (Q16W), relative to other therapies currently in use for treatment of diabetic macular oedema (DME). Of particular interest were anti-vascular endothelial growth factor (VEGF) therapies applied in flexible dosing regimens such as Pro re nata (PRN) and T&E, which are the mainstay in clinical practice.
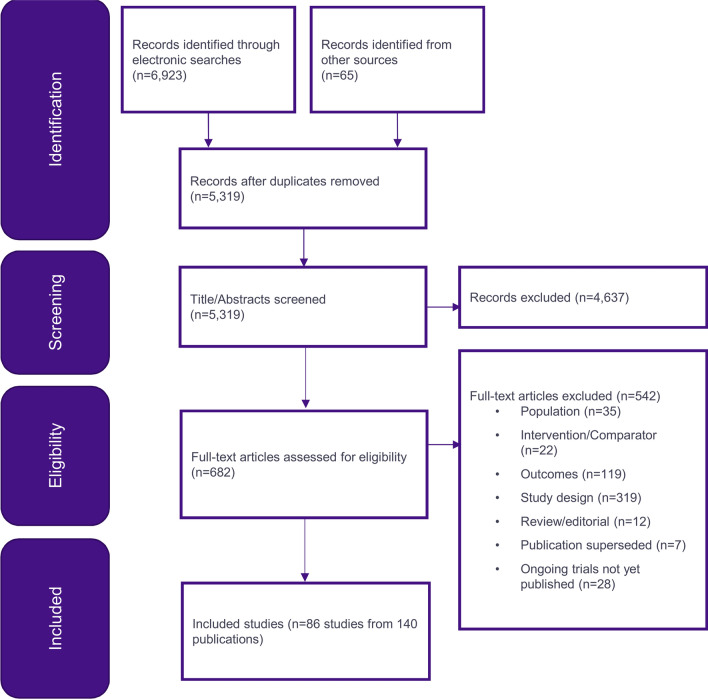
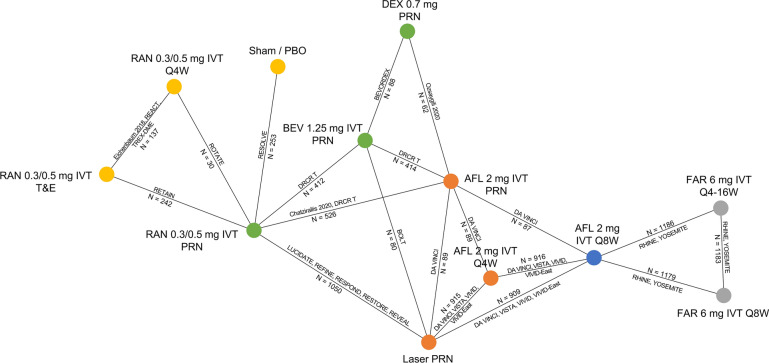
Methods: An SLR identifying randomised controlled trials (RCTs) published before August 2021 was conducted, followed by a Bayesian NMA comparing faricimab T&E treatment to aflibercept, ranibizumab, bevacizumab, dexamethasone and laser therapy. Outcomes included in the analysis were change in best-corrected visual acuity (BCVA), change in central subfield thickness (CST), injection frequency, ocular adverse events (AE) and all-cause discontinuation, all of which were evaluated at 12 months. Subgroup analyses including patients' naïve to anti-VEGF were conducted where feasible.
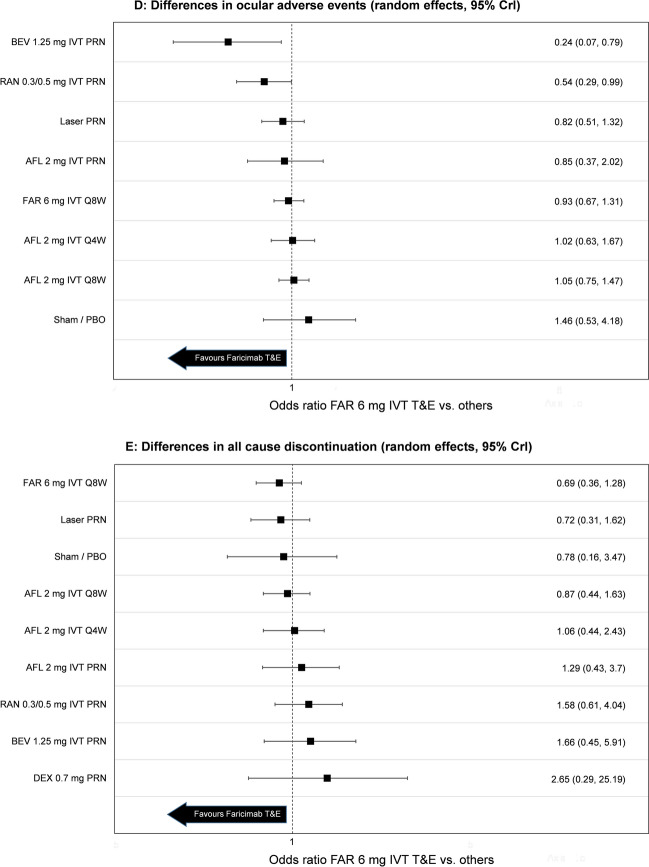
Results: Twenty-six studies identified in the SLR were included in the NMA. Most importantly for decision making in clinical practise, faricimab T&E was associated with a statistically greater (95% credible intervals exclude zero) and clinically meaningful decrease in retinal thickness compared to all other flexible dosing regimens (greater retinal drying by 55-125 microns). Anatomical outcomes determine treatment efficacy and retreatment of patients. The NMA also showed a statistically greater increase in mean change in BCVA for faricimab T&E vs. flexible regimens using ranibizumab and bevacizumab (increase of 4.4-4.8 letters) as well as a numerical improvement vs. aflibercept PRN (two letters, 95% credible intervals including zero). Accordingly, the injection frequency was numerically lower versus other treatments using flexible dosing regimens (decrease by 0.92-1.43 injections). The analyses also indicated that the safety profile of faricimab T&E was comparable to those of ranibizumab and aflibercept, which have well-established safety profiles, with similar results for the number of all-cause discontinuations.
Conclusion: Faricimab provides a new treatment option in DME with dual-pathway inhibition of VEGF and angiopoeitin-2 (Ang-2). To the authors' knowledge, this is the first indirect comparison of faricimab T&E in DME. The analyses indicate that faricimab T&E is associated with superior retinal drying along with numerically fewer injections compared to all other treatments given in flexible dosing regimens. It also showed superior visual acuity outcomes compared to ranibizumab and bevacizumab.
Keywords: Comparative efficacy; Diabetic macular oedema; Durability; Faricimab; Network meta-analysis; Safety; Systematic literature review.
© 2023. The Author(s), under exclusive licence to Springer Healthcare Ltd., part of Springer Nature.
Conflict of interest statement
Tatiana Paulo, Marloes Bagijn and Christian Bührer are employees of F. Hoffmann-La Roche Ltd. Claire Watkins is an employee of Clarostat Consulting Ltd, which was contracted by F. Hoffmann-La Roche to undertake the data analysis for this study. Nancy M. Holekamp has served as a consultant for Acucela, Allergan, Apellis, Bayer, Clearside Biosciences, Gemini, Genentech, Inc., Gyroscope, Katalyst Surgical, Lineage Cell Therapeutics, Nacuity, Notal Vision, Novartis, PolyActiva, and Regeneron, and is currently a visiting professor at F. Hoffmann-La Roche Ltd.
Figures

References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
