

Magnetic resonance detection of advanced atrial cardiomyopathy increases the risk for atypical atrial flutter occurrence following atrial fibrillation ablation
- PMID: 37751383
- PMCID: PMC10532122
- DOI: 10.1093/europace/euad276
Magnetic resonance detection of advanced atrial cardiomyopathy increases the risk for atypical atrial flutter occurrence following atrial fibrillation ablation
Abstract
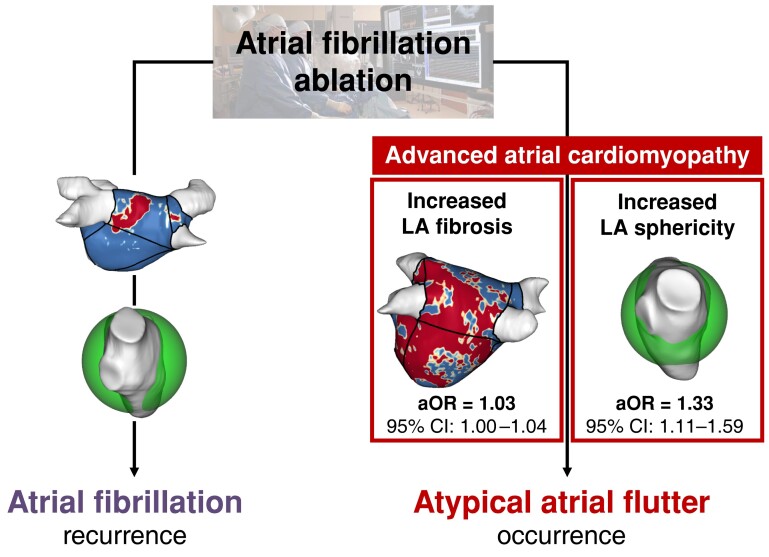
Aims: Recurrence of arrhythmia after catheter ablation of atrial fibrillation (AF) in the form of atypical atrial flutter (AFL) is common among a significant number of patients and often requires redo ablation with limited success rates. Identifying patients at high risk of AFL after AF ablation could aid in patient selection and personalized ablation approach. The study aims to assess the relationship between pre-existing atrial cardiomyopathy and the occurrence of AFL following AF ablation.
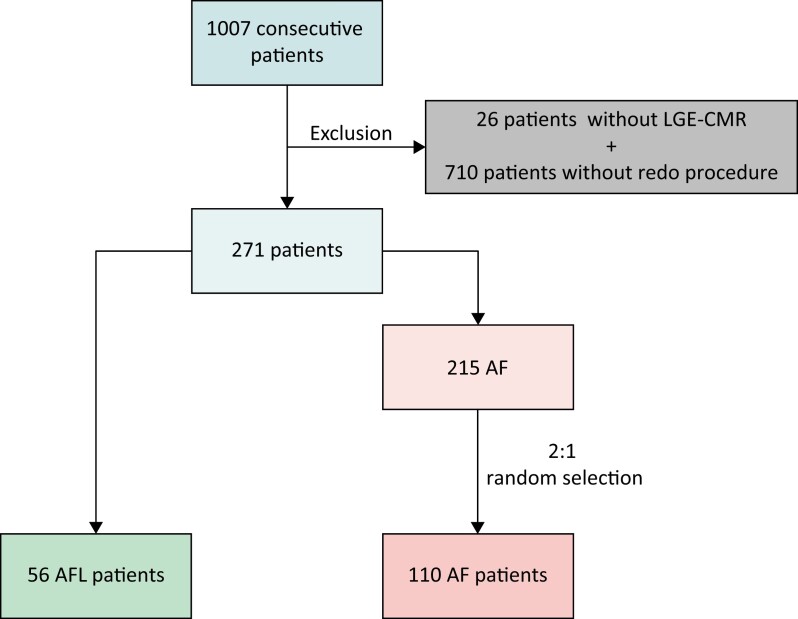
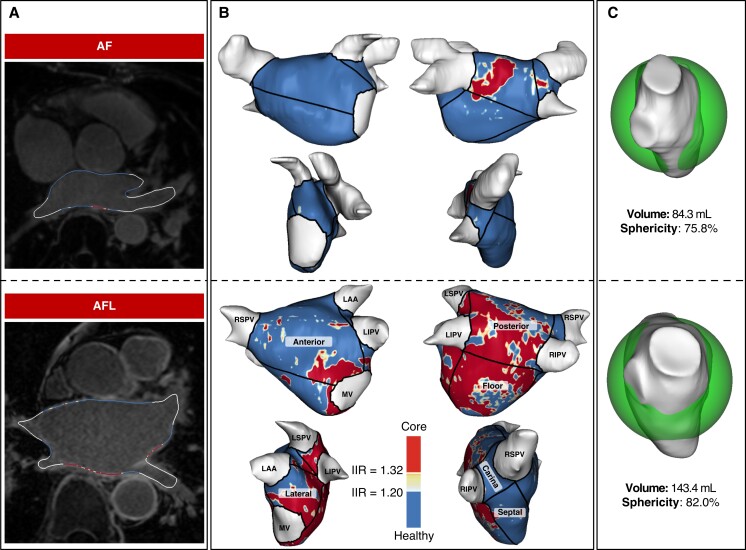
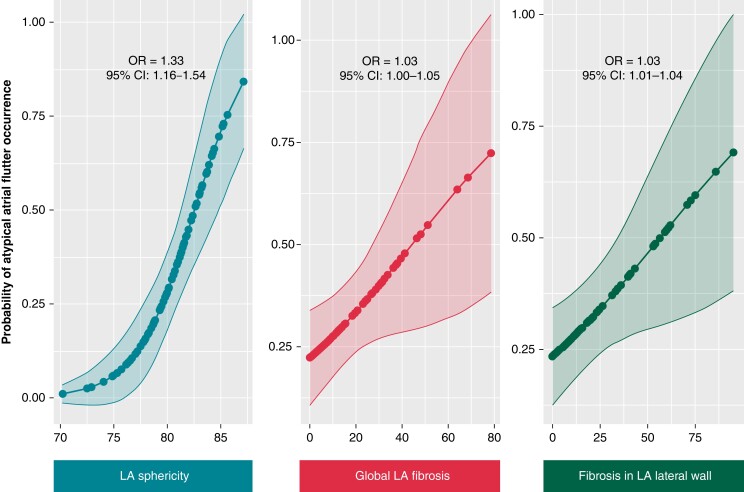
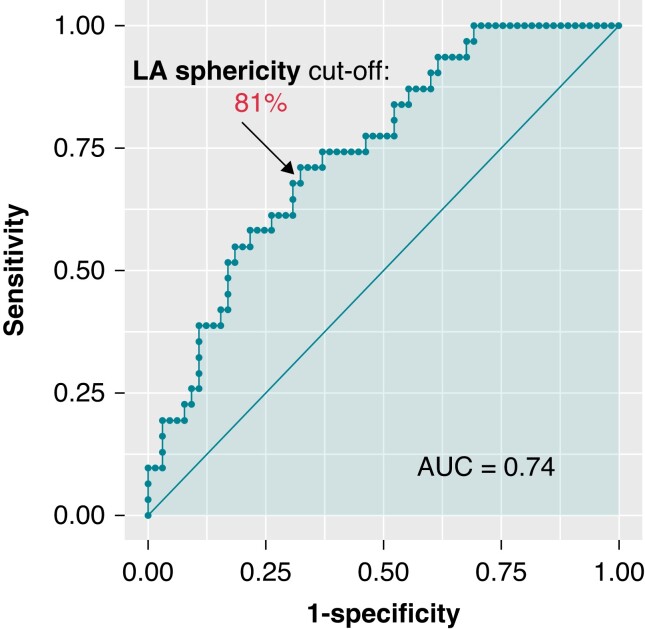
Methods and results: We analysed a cohort of 1007 consecutive AF patients who underwent catheter ablation and were included in a prospective registry. Patients who did not have baseline cardiac magnetic resonance imaging and late gadolinium enhancement (LGE-CMR) or did not experience any recurrences were excluded. A total of 166 patients were included gathering 56 patients who underwent re-ablation due to AFL recurrences and 110 patients who underwent re-ablation due to AF recurrences (P = 0.11). A multiparametric assessment of atrial cardiomyopathy was based on basal LGE-CMR, including left atrial (LA) volume, LA sphericity, and global and segmental LA fibrosis using semiautomated post-processing software. Out of the initial cohort of 1007 patients, AFL and AF occurred in 56 and 110 patients, respectively. An age higher than 65 [odds ratio (OR) = 5.6, 95% confidence interval (CI): 2.2-14.4], the number of previous ablations (OR = 3.0, 95% CI: 1.2-7.8), and the management of ablation lines in the index procedure (OR = 2.5, 95% CI: 1.0-6.3) were independently associated with AFL occurrence. Furthermore, several characteristics assessed by LGE-CMR were identified as independent predictors of AFL recurrence after the index ablation for AF, such as enhanced LA sphericity (OR = 1.3, 95% CI: 1.1-1.6), LA global fibrosis (OR = 1.03, 95% CI: 1.01-1.07), and increased fibrosis in the lateral wall (OR = 1.03, 95% CI: 1.01-1.04).
Conclusion: Advanced atrial cardiomyopathy assessed by LGE-CMR, such as increased LA sphericity, global LA fibrosis, and fibrosis in the lateral wall, is independently associated with arrhythmia recurrence in the form of AFL following AF ablation.
Keywords: Atrial cardiomyopathy; Atrial fibrillation; Atrial remodelling; Atypical atrial flutter; Fibrosis.
© The Author(s) 2023. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
References
-
- Hindricks G, Potpara T, Dagres N, Arbelo E, Bax JJ, Blomström-Lundqvist Cet al. 2020 ESC guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): the task force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur Heart J 2021;42:373–498.. - PubMed
-
- Hoyt H, Bhonsale A, Chilukuri K, Alhumaid F, Needleman M, Edwards Det al. Complications arising from catheter ablation of atrial fibrillation: temporal trends and predictors. Heart Rhythm 2011;8:1869–74. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
