

Shear wave elastography can stratify rectal cancer response to short-course radiation therapy
- PMID: 37752156
- PMCID: PMC10522682
- DOI: 10.1038/s41598-023-43383-5
Shear wave elastography can stratify rectal cancer response to short-course radiation therapy
Abstract
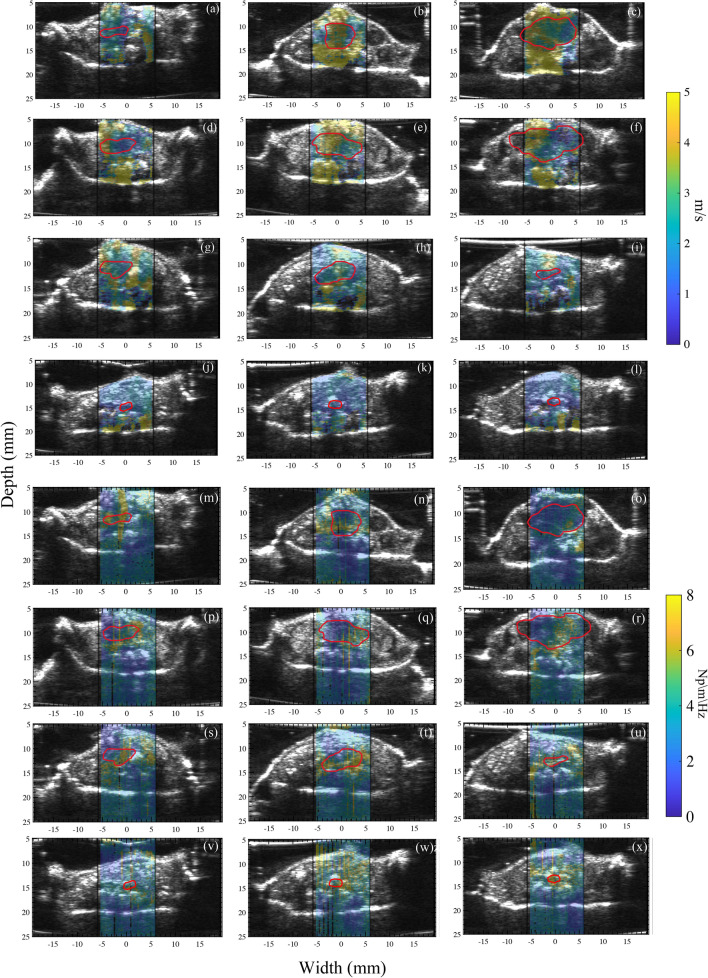
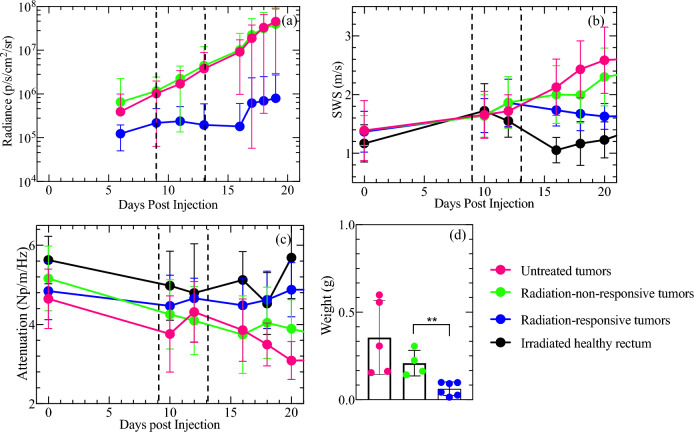
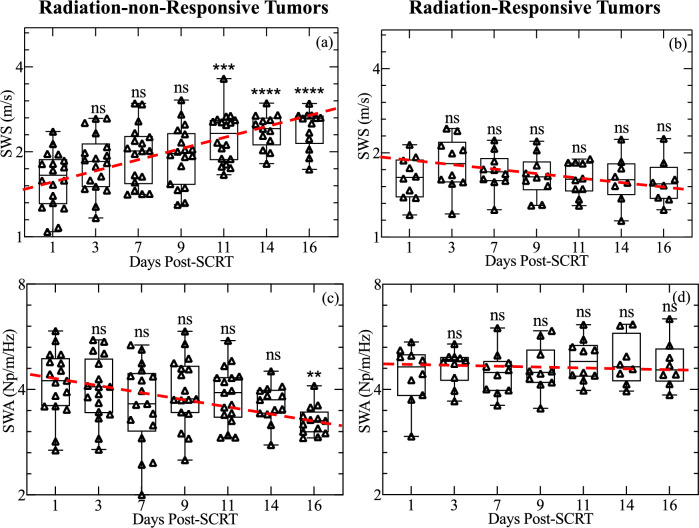
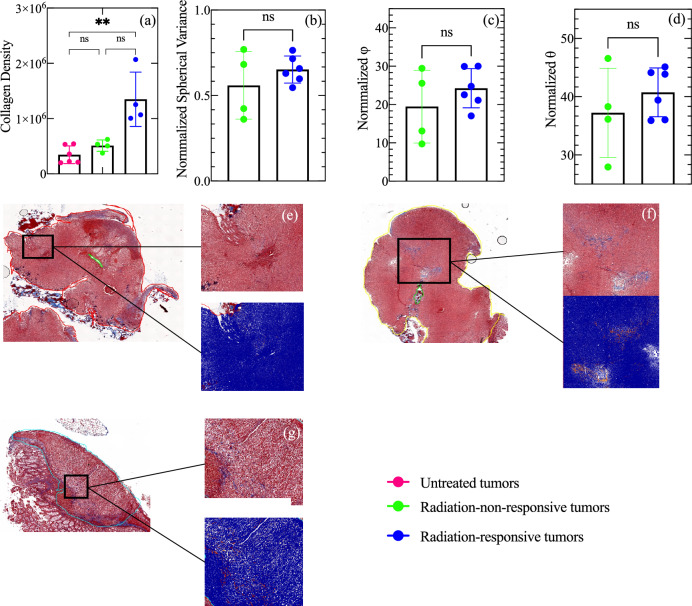
Rectal cancer is a deadly disease typically treated using neoadjuvant chemoradiotherapy followed by total mesorectal excision surgery. To reduce the occurrence of mesorectal excision surgery for patients whose tumors regress from the neoadjuvant therapy alone, conventional imaging, such as computed tomography (CT) or magnetic resonance imaging (MRI), is used to assess tumor response to neoadjuvant therapy before surgery. In this work, we hypothesize that shear wave elastography offers valuable insights into tumor response to short-course radiation therapy (SCRT)-information that could help distinguish radiation-responsive from radiation-non-responsive tumors and shed light on changes in the tumor microenvironment that may affect radiation response. To test this hypothesis, we performed elastographic imaging on murine rectal tumors (n = 32) on days 6, 10, 12, 16, 18, 20, 23, and 25 post-tumor cell injection. The study revealed that radiation-responsive and non-radiation-responsive tumors had different mechanical properties. Specifically, radiation-non-responsive tumors showed significantly higher shear wave speed SWS (p < 0.01) than radiation-responsive tumors 11 days after SCRT. Furthermore, there was a significant difference in shear wave attenuation (SWA) (p < 0.01) in radiation-non-responsive tumors 16 days after SCRT compared to SWA measured just one day after SCRT. These results demonstrate the potential of shear wave elastography to provide valuable insights into tumor response to SCRT and aid in exploring the underlying biology that drives tumors' responses to radiation.
© 2023. Springer Nature Limited.
Conflict of interest statement
The authors declare no competing interests.
Figures


References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
