

Immune cell profiles of idiopathic inflammatory myopathy patients expressed anti-aminoacyl tRNA synthetase or anti-melanoma differentiation-associated gene 5 autoantibodies
- PMID: 37752437
- PMCID: PMC10523699
- DOI: 10.1186/s12865-023-00569-w
Immune cell profiles of idiopathic inflammatory myopathy patients expressed anti-aminoacyl tRNA synthetase or anti-melanoma differentiation-associated gene 5 autoantibodies
Abstract
Background: Patients with idiopathic inflammatory myopathy (IIM) often express a different type of myositis-specific autoantibodies (MSAs), each associated with different clinical symptoms. Understanding the immunopathogenesis of various IIM subgroups can help improve the diagnosis and prognosis of IIM patients with different MSAs. However, the immune cell profiles of these IIM patients with anti-aminoacyl tRNA synthetase (ARS) or anti-melanoma differentiation-associated gene 5 (MDA5) autoantibodies remain unclear. We focused on the immune cell profiles of IIM patients with anti-ARS or anti-MDA5 autoantibodies.
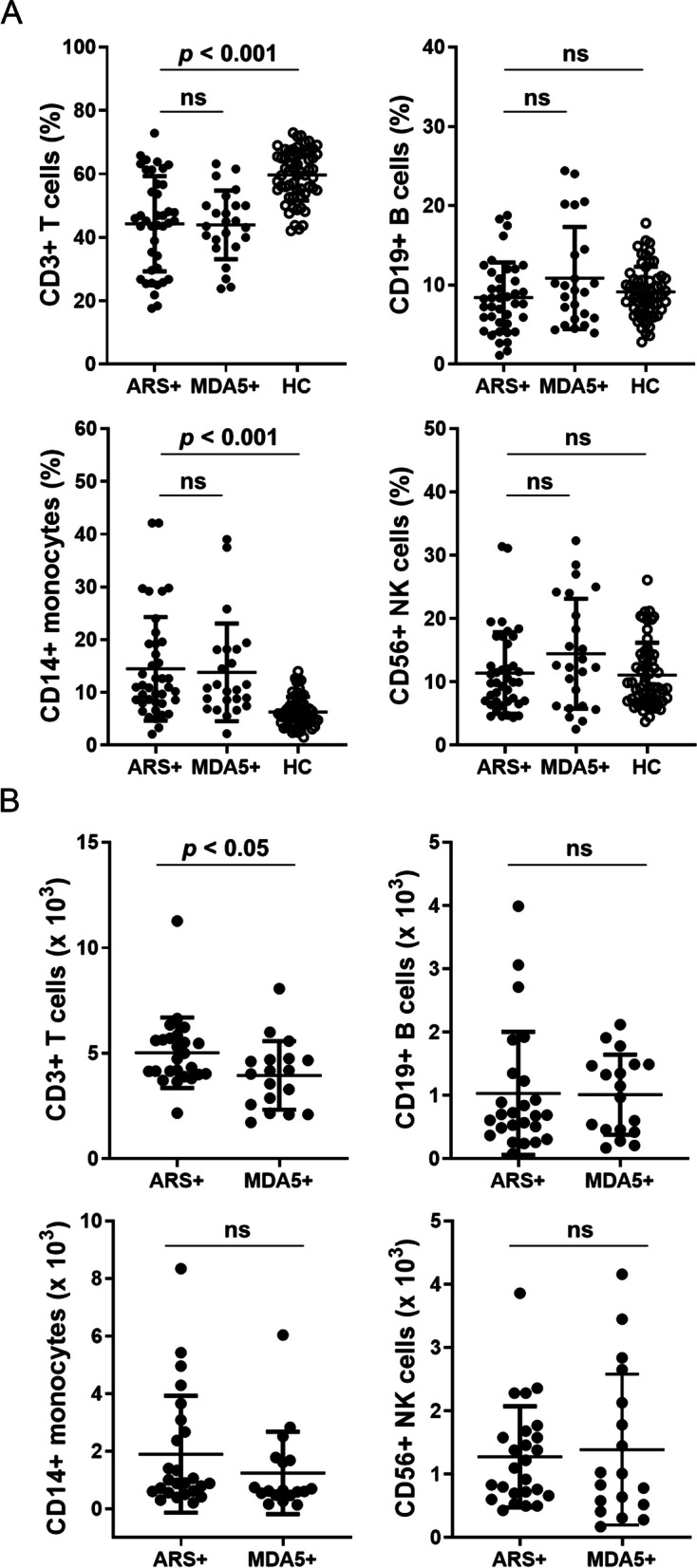
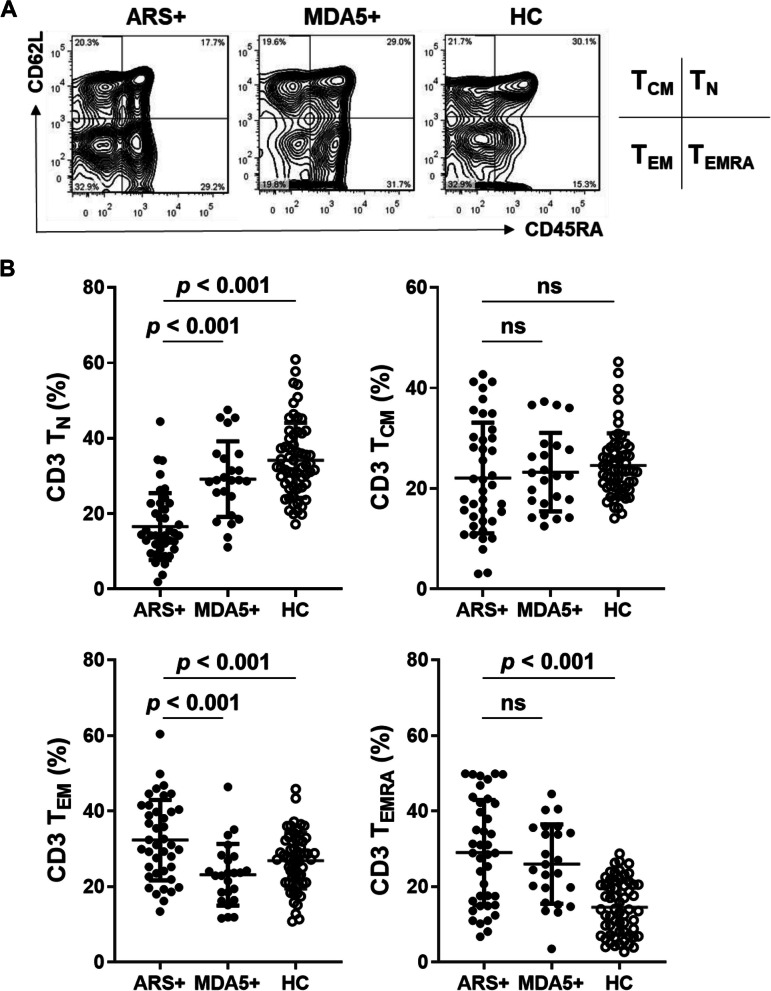
Results: The peripheral blood from IIM patients with anti-MDA5 autoantibody (MDA5 + group, n = 24) or one of the anti-ARS autoantibodies (ARS + group, n = 40) autoantibodies, and healthy controls (HC group, n = 60) were collected and examined. We found that IIM patients had a lower CD3 T cell population compared to the HC group. IIM patients showed a significantly lower TN cell population and a higher TEMRA cell population. Higher Th17 and Treg cell populations were found in these IIM patients than in the HC group. In these IIM patients, the MDA5 + group exhibited the higher percentages of Th17 and Treg cells than the ARS + group. It is noteworthy that the percentage of Th1 cells in the survival subgroup was higher than in the death subgroup in IIM patients with ARS + or MDA5 + . Furthermore, in the MDA5 + group, the percentage of Treg cells was higher in the survival subgroup compared to the death subgroup.
Conclusions: Our study demonstrated that elevated Th1 may be a good prognostic indicator in IIM patients with ARS + or MDA5 + . Elevated Treg may also help predict a good prognosis in MDA5 + IIM patients. However, more large-scale studies and clinical samples are needed to verify the significance of Th1 and Treg cell subsets in clinical outcomes for these IIM patients with ARS + or MDA5 + . These data may help design a therapeutic approach that specifically targets the pathogenic immune molecular responsible for autoimmune attacks in IIM.
Keywords: Aminoacyl-tRNA synthetase (ARS); Idiopathic inflammatory myositis (IIM); Immune cell profiles; Melanoma differentiation-associated gene 5 (MDA5); Myositis-specific autoantibody (MSA).
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures



References
-
- Cheeti A, Brent LH, Panginikkod S: Autoimmune Myopathies. In: StatPearls. edn. Treasure Island (FL): StatPearls Publishing Copyright © 2023, StatPearls Publishing LLC.; 2023.
-
- Sarwar A, Dydyk AM, Jatwani S. Polymyositis. In: StatPearls. edn. Treasure Island (FL): StatPearls Publishing LLC; 2023. StatPearls Publishing Copyright © 2023.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
