

Treat-to-target strategies for the management of familial Mediterranean Fever in children
- PMID: 37752496
- PMCID: PMC10521475
- DOI: 10.1186/s12969-023-00875-y
Treat-to-target strategies for the management of familial Mediterranean Fever in children
Abstract
Background: The objective of this initiative was to develop a treat-to-target (T2T) approach for the management of patients with Familial Mediterranean Fever (FMF), including the definition of a complex treatment target, and establish strategies that improve patient care and long-term outcome.
Methods: An initial set of statements as well as a flow chart visualising the proposed concept was developed. To adapt the preliminary statements to the current state of knowledge, a systematic literature search was performed and the modified statements were subject to a Delphi approach. To ensure the applicability of the statements in daily practice, an online survey was conducted among paediatric rheumatologists in Germany. In addition, data from the national AID-NET registry were analysed with respect to therapeutic response.
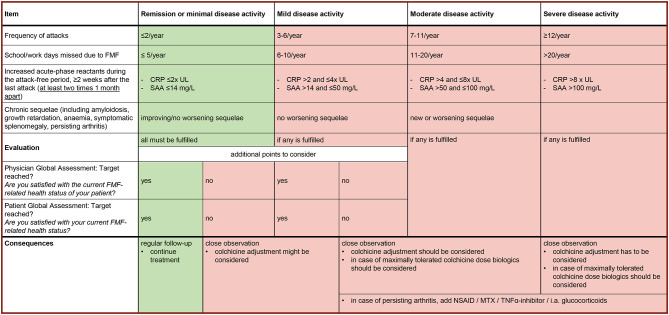
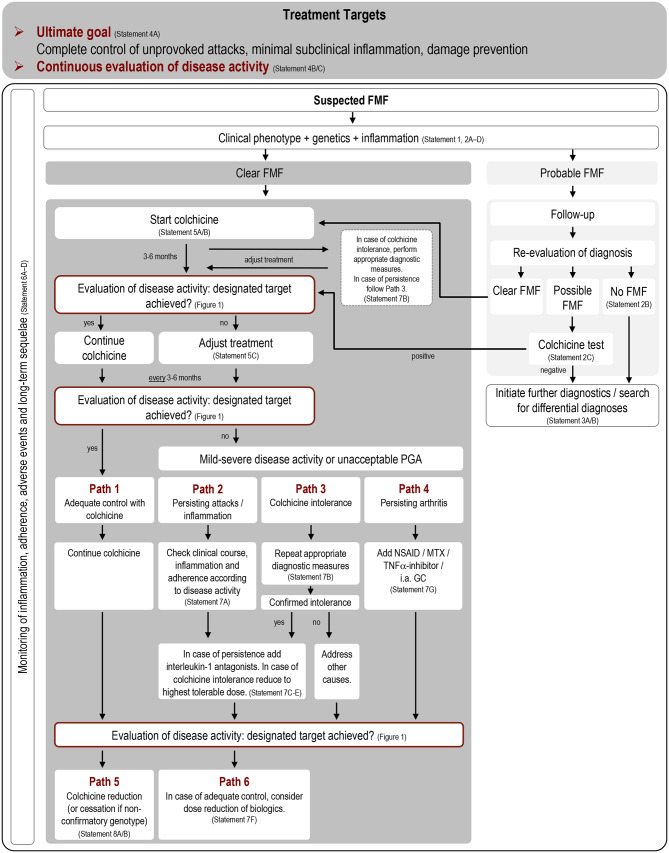
Results: This T2T initiative yielded a total of 26 statements guiding FMF management with respect to diagnosis, treatment targets, treatment strategies and monitoring. The online survey identified cut-off values for inflammatory markers indicating treatment intensification and appropriate measures in case of colchicine intolerance or non-adherence. The analysis of data derived from the national AID-NET showed that colchicine therapy was successfully terminated in 61% of patients (27 out of 44) with heterozygous MEFV mutations. Multidimensional treatment targets incorporating objective and subjective reported outcome measures were developed. These provide the basis for stratifying patients into the following treatment paths: continue colchicine, persisting attacks / inflammation, colchicine intolerance, persisting arthritis, colchicine reduction and adjustment/reduction of biologics.
Conclusions: The proposed consensus treatment plan for the management of FMF incorporates multidimensional targets allowing transparent treatment decisions, which will promote personalised disease management and increase adherence to therapy.
Keywords: Children; Colchicine; Colchicine resistance; Disease activity; Familial Mediterranean Fever; Medication adherence; Treat-to-target; interleukin-1 antagonists.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
Lisa Ehlers has no conflicts of interest to declare. Elisabeth Rolfes has no conflicts of interest to declare. Mareike Lieber is a member of the following medical society: GKJR. Dominik Müller has no conflicts of interest to declare. Elke Lainka received consulting fees from Mirum and Albireo. Faekah Gohar has no conflicts of interest to declare. Günter Klaus has no conflicts of interest to declare. Hermann Girschick was involved in the development of treatment guidelines of the following societies: DGKJ. Jana Hörstermann has no conflicts of interest to declare. Jasmin Kümmerle-Deschner received consulting fees, honoraria and research grants from Novartis and SOBI, and is a member of the following medical societies: GKJR, DGRh, PRES, ISSAID. Jürgen Brunner received honoraria for presenting at industrial symposia and is a member of the following medical societies: DGKJ, ÖGKJ, ÖGR, GKJR, DGPI. Katharina Palm-Beden has no conflicts of interest to declare. Klaus Tenbrock received consulting fees from Pfizer and Novartis, a research grant from Pfizer, and was involved in the development of treatment guidelines of the following societies: GKJR. Lusine von Wrangel has no conflicts of interest to declare. Maria Faßhauer has no conflicts of interest to declare. Norbert Blank received consulting fees, honoraria and research grants from Novartis and SOBI, and is a member of the following medical societies: DGRh, DNSS, ISA. Ralf Trauzeddel received consulting fees from Novartis and was involved in the development of a treatment guideline of the following society: AWMF. Anne Sae Lim von Stuckrad has no conflicts of interest to declare. Sonja Higgins has no conflicts of interest to declare. Tatjana Welzel has no conflicts of interest to declare. Thomas Lutz is a member of the following medical societies: GKJR, DGKJ, DGPI. Véronique Hentgen has received consulting fees and honoraria from Novartis and SOBI, is a member of the steering committee of the JIRcohort which received public and private funding for research, and is involved in the development of French guidelines on behalf of the Haute Autorité de Santé (HAS). She is a member of the following medical societies:SOFREMIP, PReS and ISSAID. Dirk Foell received research funding from Novartis and Sobi, honoraria from Novartis and Sobi, and is a member of the following medical societies: GKJR, API, ISSAID, PReS, GPGE, and DGKJ. Helmut Wittkowski received research funding from Takeda, honoraria from Novartis and Takeda, travel grants from Octapharma and CSL-Behring, and is a member of the following medical societies: GKJR, API. Tilmann Kallinich is a member of the following medical societies: GKJR and DGPI.
Figures
References
-
- Schwartz DM, Kitakule MM, Dizon BL, et al. Systematic evaluation of nine monogenic autoinflammatory diseases reveals common and disease-specific correlations with allergy-associated features. Ann Rheum Dis Published Online First: 22 February. 2021 doi: 10.1136/annrheumdis-2020-219137. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
