

Endovascular therapy versus best medical management for isolated posterior cerebral artery occlusion: A systematic review and meta-analysis
- PMID: 37752802
- PMCID: PMC10916830
- DOI: 10.1177/23969873231201715
Endovascular therapy versus best medical management for isolated posterior cerebral artery occlusion: A systematic review and meta-analysis
Abstract
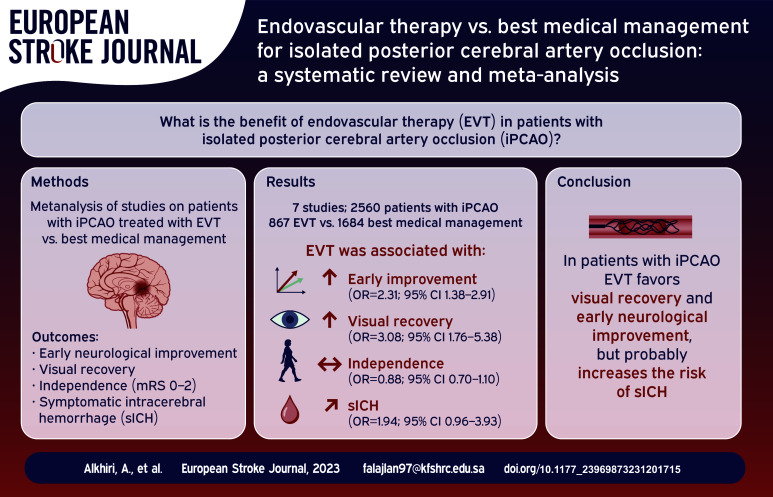
Background and purpose: Isolated posterior cerebral artery occlusions (iPCAO) were underrepresented in pivotal randomized clinical trial (RCTs) of endovascular thrombectomy (EVT) in ischemic stroke, and the benefit of EVT in this population is still indeterminate. We performed a systematic review and a meta-analysis to compare the safety and efficacy of EVT compared to best medical management (BMM) in patients with iPCAO.
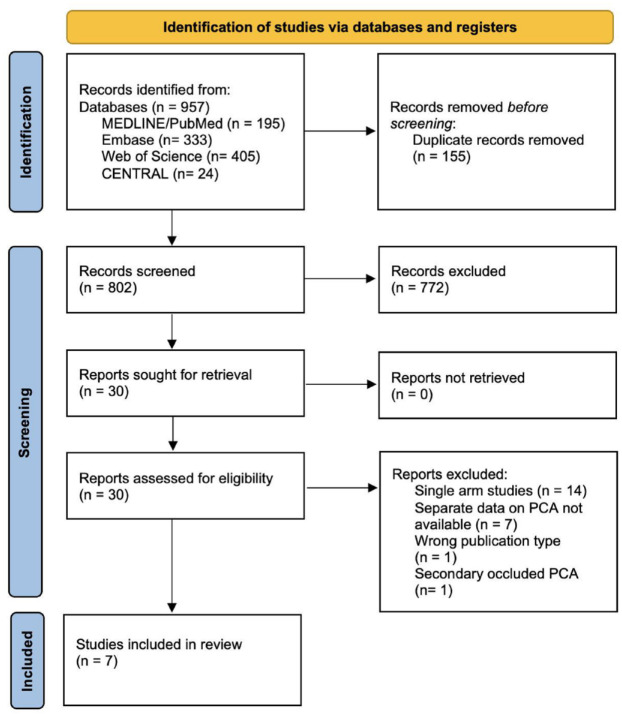
Methods: We searched Medline/PubMed, Embase, Web of Science, and the Cochrane databases up to May 2023 for eligible studies reporting outcomes of patients with iPCAO treated with EVT or BMM. We pooled odds ratios (ORs) with corresponding 95% confidence intervals (CI) using a random-effects model.
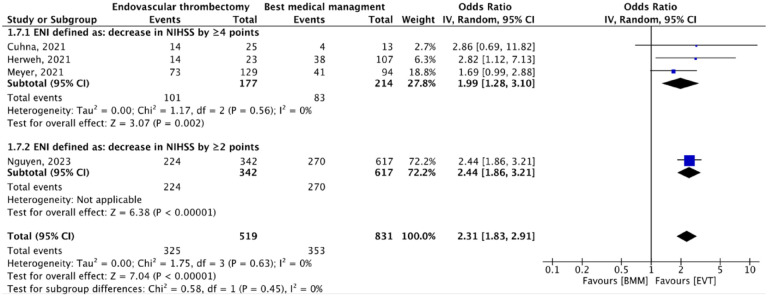
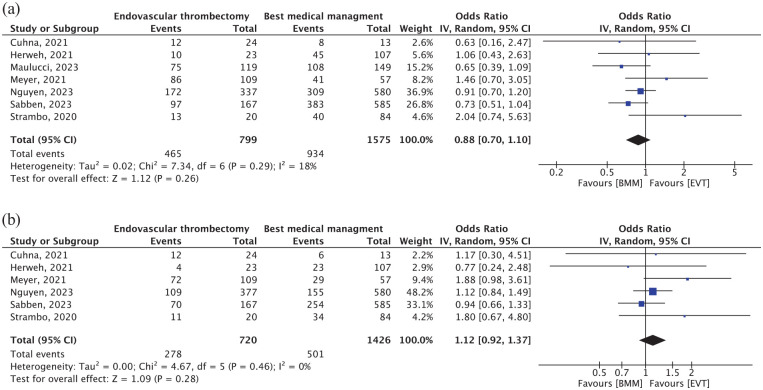
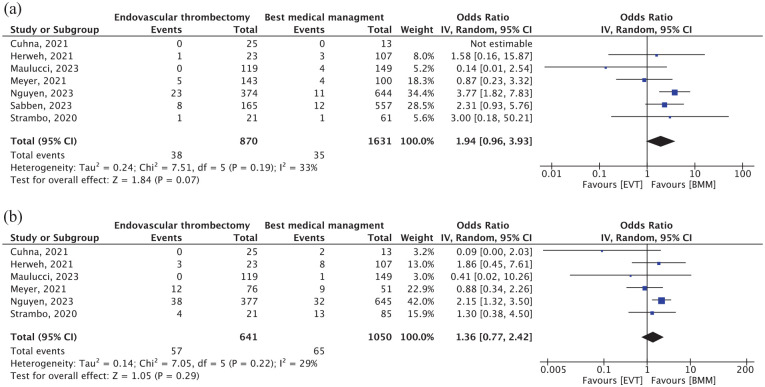
Results: Seven studies involving 2560 patients were included. EVT was associated with significantly higher likelihood of early neurological improvement (OR, 2.31 [95% CI, 1.38-2.91]; p < 0.00001) and visual field normalization (OR, 3.08 [95% CI, 1.76-5.38]; p < 0.0001) compared to BMM. Rates of good functional outcomes (mRS 0-2) were comparable between the two arms (OR, 0.88 [95% CI, 0.70-1.10]; p = 0.26). Symptomatic intracranial hemorrhage (sICH) was comparable between the two groups (OR, 1.94 [95% CI, 0.96-3.93]; p = 0.07). Mortality was also similar between the two groups (OR, 1.36; [95% CI, 0.77-2.42]; p = 0.29).
Conclusions: In patients with iPCAO, EVT was associated with visual and early neurological improvement but with a strong trend toward increased sICH. Survival and functional outcomes may be slightly poorer. The role of EVT in iPCAO remains uncertain.
Keywords: Posterior cerebral artery; ischemic stroke; meta-analysis; thrombectomy.
Conflict of interest statement
Declaration of conflicting interestsThe author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures

References
-
- Ntaios G, Spengos K, Vemmou AM, et al.. Long-term outcome in posterior cerebral artery stroke. Eur J Neurol 2011; 18: 1074–1080. - PubMed
-
- Cunha B, Baptista M, Pamplona J, et al.. Acute treatment of isolated posterior cerebral artery occlusion: single center experience. J Stroke Cerebrovasc Dis 2022; 31: 106239. - PubMed
-
- Strambo D, Bartolini B, Beaud V, et al.. Thrombectomy and thrombolysis of isolated posterior cerebral artery occlusion: cognitive, visual, and disability outcomes. Stroke 2020; 51: 254–261. - PubMed
-
- Brandt T, Steinke W, Thie A, et al.. Posterior cerebral artery territory infarcts: clinical features, infarct topography, causes and outcome. Multicenter results and a review of the literature. Cerebrovasc Dis 2000; 10: 170–182. - PubMed
-
- Ng YS, Stein J, Salles SS, et al.. Clinical characteristics and rehabilitation outcomes of patients with posterior cerebral artery stroke. Arch Phys Med Rehabil 2005; 86: 2138–2143. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
