

Meta-Analysis of Rates and Risk Factors for Local Recurrence in Surgically Resected Patients With NSCLC and Differences Between Asian and Non-Asian Populations
- PMID: 37753322
- PMCID: PMC10518711
- DOI: 10.1016/j.jtocrr.2023.100515
Meta-Analysis of Rates and Risk Factors for Local Recurrence in Surgically Resected Patients With NSCLC and Differences Between Asian and Non-Asian Populations
Abstract
Introduction: Postoperative radiotherapy (PORT) reduces local failure in patients with NSCLC, without a clear overall survival benefit. It is unknown whether the subsets of patients benefit. Two recent large randomized controlled trials, PORT-C (People's Republic of China) and Lung ART (Europe), reported widely different locoregional recurrence (LR) rates in the control arms, at 18.3% and 28.1% (46% of which were mediastinal recurrences), respectively. We performed a meta-analysis of patients with pathologic (p) N0 to N2 disease to evaluate the risk factors for LR and to explore possible differences in recurrence risk between Asian population (AP) and non-Asian population (NAP).
Methods: We identified all original studies of curative NSCLC surgical resection which reported risk of LR between January 1, 2000, and January 10, 2021, excluding studies with less than 10 LR, patients with metastatic disease, or any neoadjuvant therapy. A total of 87 studies were identified with pN0 to N2 disease; of these, 56 were of high quality (HQ) on the basis of the Newcastle-Ottawa Scale. For each risk factor, we derived pooled relative risk (RR) and 5-year rate estimates using random-effects models.
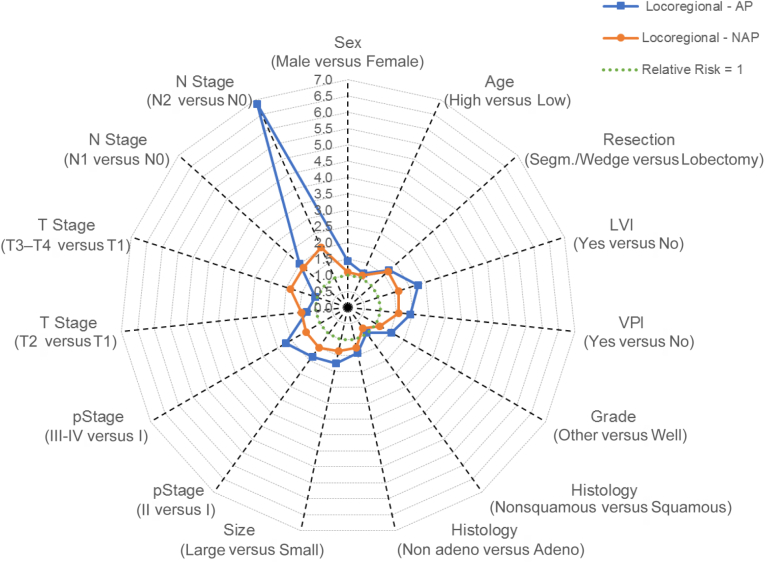
Results: Overall, the three significant highest pooled RRs (95% confidence intervals) for LR were pN2 versus pN0 (3.01, 1.39-6.55), lymphovascular invasion (1.92, 1.58-2.33), and advanced pT3-4 stage versus pT1 (1.86, 1.53-2.25). For HQ studies, the highest RRs for LR were lymphovascular invasion (1.94, 1.57-2.40), sublobar versus lobar resection (1.86, 1.46-2.36), and pN1 versus pN0 (1.84, 1.37-2.47), but pN2 versus pN0 was no longer significant (3.0, 0.57-15.61), on the basis of only two eligible studies. The RRs for LR were consistent for most factors in AP and NAP, although the RR for male versus female sex was higher in AP (1.44, 1.21-1.72) than in NAP (1.09, 0.99-1.19). Where reported, the pooled rate of LR at 5 years was lower in AP (12.0%) than in NAP (22.7%), despite similar overall 5-year recurrence rates (both LR and distal) in both populations: 38.0% in AP and 37.3% in NAP. Nevertheless, a lower 5-year mortality rate was noted in AP (24.3%) than in NAP (45.9%).
Conclusions: There is little high-quality evidence to support the hypothesis that pN2 disease is a risk factor for LR, but LR seems to be lower in Asians. Prospective evaluation of LR factors and rates may be necessary before further prospective evaluation of PORT, because it may not depend on nodal status alone. Recurrence rates may differ in Asians. The impact of mutational status and modern treatment including targeted therapies and immune checkpoint inhibitors is inadequately studied.
Keywords: Locoregional recurrence; Meta-analysis; Non–small cell lung cancer; Recurrence rates; Risk factors; Surgical resection.
© 2023 The Authors.
Figures

Similar articles
-
Risk factors for locoregional recurrence in patients with resected N1 non-small cell lung cancer: a retrospective study to identify patterns of failure and implications for adjuvant radiotherapy.Radiat Oncol. 2013 Dec 9;8:286. doi: 10.1186/1748-717X-8-286. Radiat Oncol. 2013. PMID: 24321392 Free PMC article.
-
Nodal stage of surgically resected non-small cell lung cancer and its effect on recurrence patterns and overall survival.Int J Radiat Oncol Biol Phys. 2015 Mar 15;91(4):765-73. doi: 10.1016/j.ijrobp.2014.12.028. Int J Radiat Oncol Biol Phys. 2015. PMID: 25752390
-
Resected pN1 non-small cell lung cancer: recurrence patterns and nodal risk factors may suggest selection criteria for post-operative radiotherapy.Radiol Med. 2016 Sep;121(9):696-703. doi: 10.1007/s11547-016-0648-z. Epub 2016 May 26. Radiol Med. 2016. PMID: 27230669
-
Indications and Parameters Around Postoperative Radiation Therapy for Lung Cancer.J Clin Oncol. 2022 Feb 20;40(6):556-566. doi: 10.1200/JCO.21.01774. Epub 2022 Jan 5. J Clin Oncol. 2022. PMID: 34985927 Review.
-
Modern post-operative radiotherapy for stage III non-small cell lung cancer may improve local control and survival: a meta-analysis.Radiother Oncol. 2014 Jan;110(1):3-8. doi: 10.1016/j.radonc.2013.08.011. Epub 2013 Oct 4. Radiother Oncol. 2014. PMID: 24100149 Review.
Cited by
-
Lymphatic vascular invasion: Diagnostic variability and overall survival impact on patients undergoing surgical resection.JTCVS Open. 2024 Aug 31;21:313-340. doi: 10.1016/j.xjon.2024.08.012. eCollection 2024 Oct. JTCVS Open. 2024. PMID: 39534344 Free PMC article.
References
-
- Hsu C.P., Hsia J.Y., Chang G.C., et al. Surgical-pathologic factors affect long-term outcomes in stage IB (pT2 N0 M0) non-small cell lung cancer: a heterogeneous disease. J Thorac Cardiovasc Surg. 2009;138:426–433. - PubMed
-
- Chansky K., Sculier J.P., Crowley J.J., et al. The International Association for the Study of Lung Cancer Staging Project: prognostic factors and pathologic TNM stage in surgically managed non-small cell lung cancer. J Thor Oncol. 2009;4:792–801. - PubMed
-
- Rotolo F., Dunant A., LeChevalier T., Pignon J.P., Arriagada R., IALT Collaborative Group Adjuvant cisplatin-based chemotherapy in nonsmall-cell lung cancer: new insights into the effect on failure type via a multistate approach. Ann Oncol. 2014;25:2162–2166. - PubMed
-
- Ginsberg R.J., Rubenstein L.V. Randomized trial of lobectomy versus limited resection for T1 N0 non-small cell lung cancer. Lung Cancer Study Group. Ann Thor Surg. 1995;60:615–623. - PubMed
-
- Gagliasso M., Migliaretti G., Ardissone F. Assessing the prognostic impact of the International Association for the Study of Lung Cancer proposed definitions of complete, uncertain, and incomplete resection in non-small cell lung cancer surgery. Lung Cancer. 2017;111:124–130. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
