

Early Omicron infection is associated with increased reinfection risk in older adults in long-term care and retirement facilities
- PMID: 37753447
- PMCID: PMC10518514
- DOI: 10.1016/j.eclinm.2023.102148
Early Omicron infection is associated with increased reinfection risk in older adults in long-term care and retirement facilities
Abstract
Background: Older adults are at increased risk of SARS-CoV-2 Omicron infection and severe disease, especially those in congregate living settings, despite high SARS-CoV-2 vaccine coverage. It is unclear whether hybrid immunity (combined vaccination and infection) after one Omicron infection provides increased protection against subsequent Omicron reinfection in older adults.
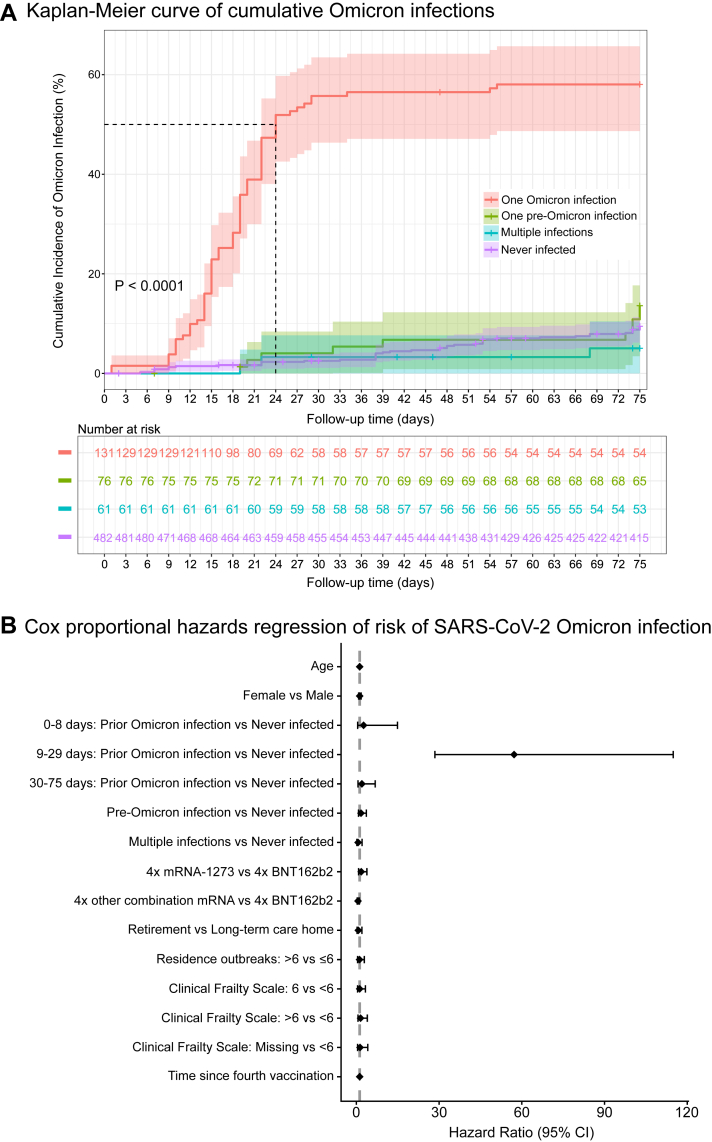
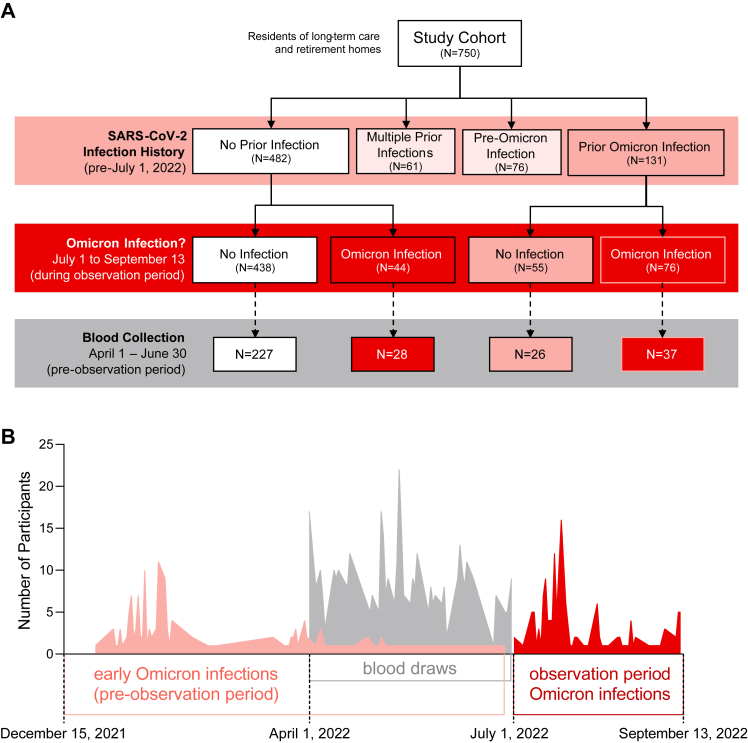
Methods: Incidence of SARS-CoV-2 Omicron infection was examined in 750 vaccinated residents of long-term care and retirement homes in the observational cohort COVID in Long-Term Care Study in Ontario, Canada, within a 75-day period (July to September 2022). Risk of infection was assessed by Cox proportional hazards regression. Serum anti-spike and anti-RBD SARS-CoV-2 IgG and IgA antibodies, microneutralization titres, and spike-specific T cell memory responses, were examined in a subset of 318 residents within the preceding three months.
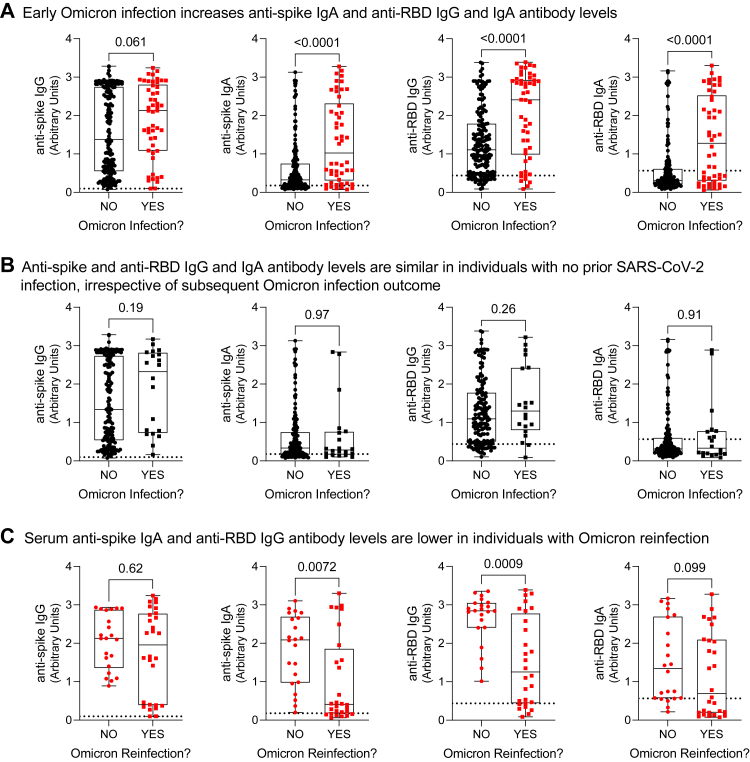
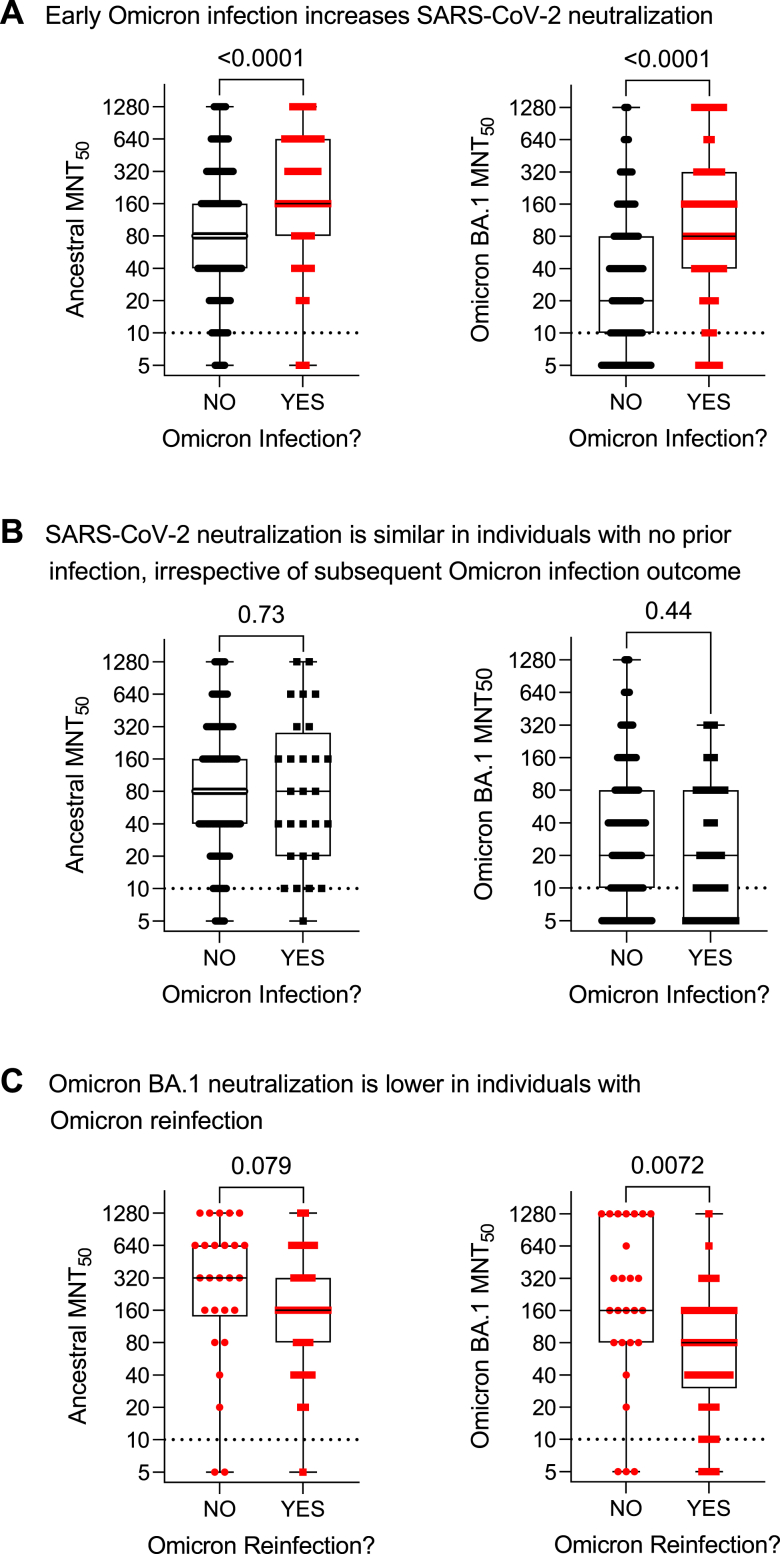
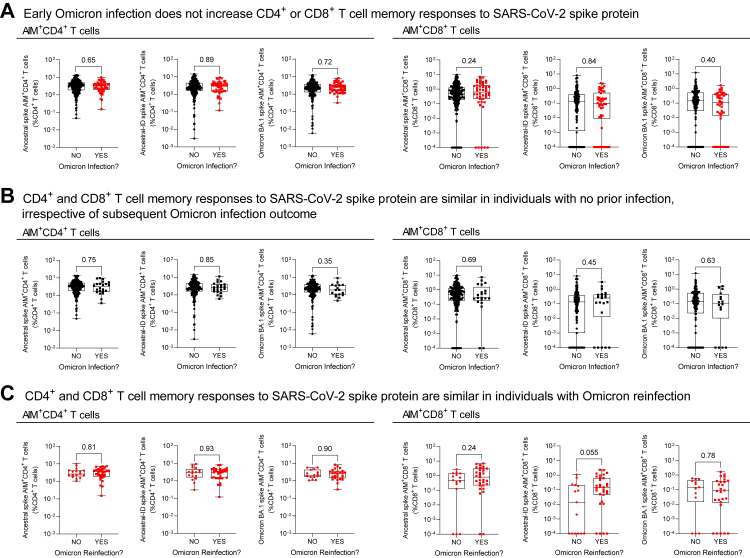
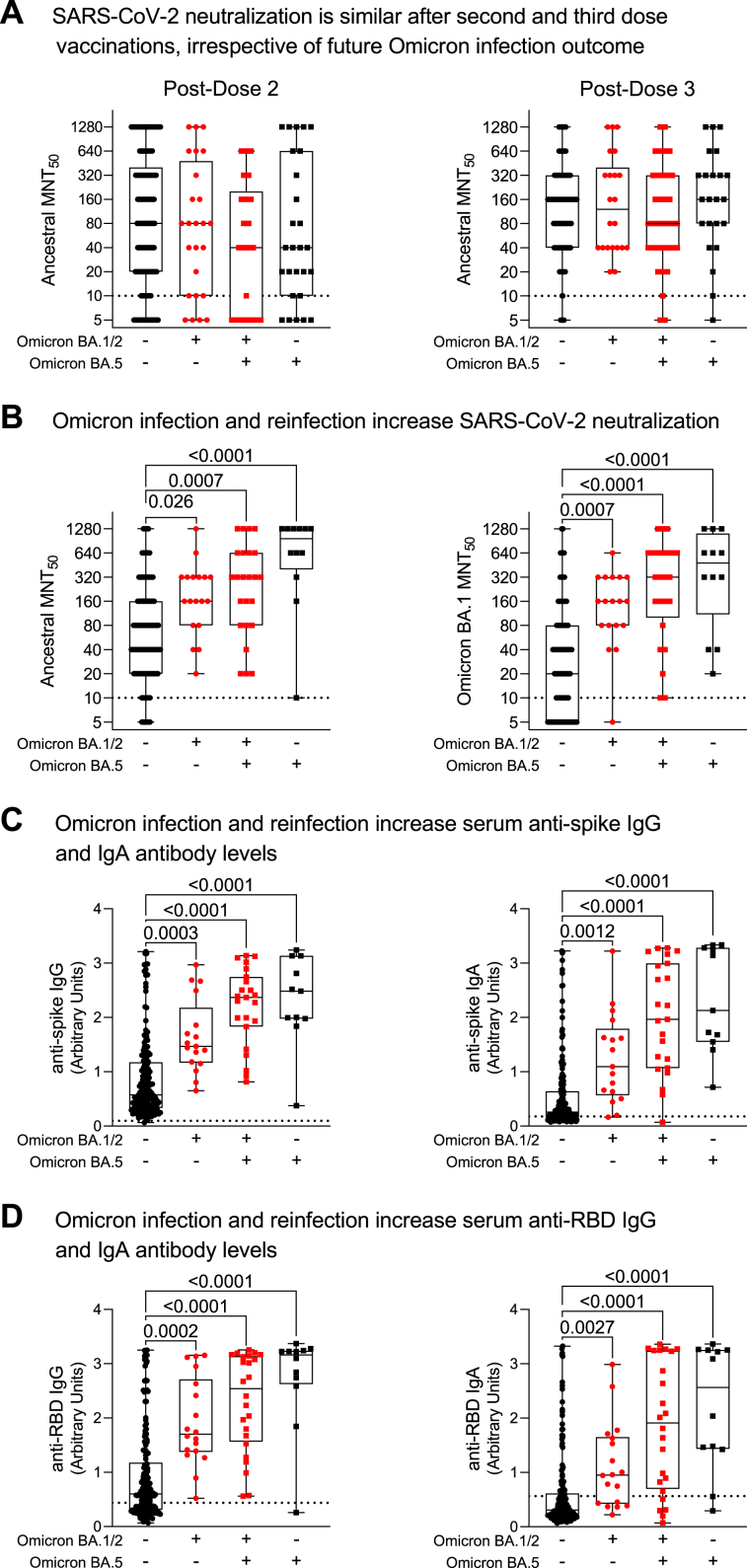
Findings: 133 of 750 participants (17.7%) had a PCR-confirmed Omicron infection during the observation period. Increased infection risk was associated with prior Omicron infection (at 9-29 days: 47.67 [23.73-95.76]), and this was not attributed to days since fourth vaccination (1.00 [1.00-1.01]) or residence outbreaks (>6 compared to ≤6: 0.95 [0.37-2.41]). Instead, reinfected participants had lower serum neutralizing antibodies to ancestral and Omicron BA.1 SARS-CoV-2, and lower anti-RBD IgG and IgA antibodies, after their initial Omicron infection.
Interpretation: Counterintuitively, SARS-CoV-2 Omicron infection was associated with increased risk of Omicron reinfection in residents of long-term care and retirement homes. Less robust humoral hybrid immune responses in older adults may contribute to risk of Omicron reinfection.
Funding: COVID-19 Immunity Task Force of the Public Health Agency of Canada.
Keywords: COVID-19; Hybrid immunity; Older adults; Omicron; SARS-CoV-2.
© 2023 The Author(s).
Conflict of interest statement
TK has received funding from the COVID-19 Immunity Task Force of the Public Health Agency of Canada to attend a conference of the COVID-19 Immunity Task Force. MSM has received research grants from Providence Therapeutics, Medicago, Bay Area Health Trust, and Lactiga, and honoraria for speaking at Boehringer Ingelheim and development of COVOICES Educational Initiatives at Sanofi, as well as consulting fees from Seqirus, Sanofi, and Grifols, has patents in unrelated technology, holds stock with Aeroimmune Biotherapeutics and stock options with Kapoose Creek Wellness, and is a member of the COVID-19 working group of the National Advisory Committee on Immunization (NACI). APC has received other research funding from the COVID-19 Immunity Task Force of the Public Health Agency of Canada. DMEB has received honoraria from AstraZeneca Mexico for a lecture, consulting fees from Pfizer and AstraZeneca, and holds a volunteer position on the Board of Directors of the Ontario Lung Health Foundation. All other authors declare no competing interests.
Figures
Similar articles
-
Early humoral and cellular responses after bivalent SARS-CoV-2 mRNA-1273.214 vaccination in long-term care and retirement home residents in Ontario, Canada: An observational cohort study.J Med Virol. 2023 Oct;95(10):e29170. doi: 10.1002/jmv.29170. J Med Virol. 2023. PMID: 37822054
-
Minimal Impact of Prior Common Cold Coronavirus Exposure on Immune Responses to Severe Acute Respiratory Syndrome Coronavirus 2 Vaccination or Infection Risk in Older Adults in Congregate Care.Open Forum Infect Dis. 2025 May 1;12(5):ofaf178. doi: 10.1093/ofid/ofaf178. eCollection 2025 May. Open Forum Infect Dis. 2025. PMID: 40313478 Free PMC article.
-
Protection from Omicron Infection in Residents of Nursing and Retirement Homes in Ontario, Canada.J Am Med Dir Assoc. 2023 May;24(5):753-758. doi: 10.1016/j.jamda.2023.02.105. Epub 2023 Mar 28. J Am Med Dir Assoc. 2023. PMID: 37001559 Free PMC article.
-
Past SARS-CoV-2 infection protection against re-infection: a systematic review and meta-analysis.Lancet. 2023 Mar 11;401(10379):833-842. doi: 10.1016/S0140-6736(22)02465-5. Epub 2023 Feb 16. Lancet. 2023. PMID: 36930674 Free PMC article.
-
Role of previous infection with SARS-CoV-2 in protecting against omicron reinfections and severe complications of COVID-19 compared to pre-omicron variants: a systematic review.BMC Infect Dis. 2023 Jun 26;23(1):432. doi: 10.1186/s12879-023-08328-3. BMC Infect Dis. 2023. PMID: 37365490 Free PMC article.
Cited by
-
Dried Cannabis Use, Tobacco Smoking, and COVID-19 Infection: Findings from a Longitudinal Observational Cohort Study.Cannabis. 2024 Dec 12;7(3):177-192. doi: 10.26828/cannabis/2024/000248. eCollection 2024. Cannabis. 2024. PMID: 39781558 Free PMC article.
-
Identification of Clinical and Genomic Features Associated with SARS-CoV-2 Reinfections.Viruses. 2025 Jun 11;17(6):840. doi: 10.3390/v17060840. Viruses. 2025. PMID: 40573431 Free PMC article.
-
Rapid Emergence and Evolution of SARS-CoV-2 Intrahost Variants among COVID-19 Patients with Prolonged Infections, Singapore.Emerg Infect Dis. 2025 Aug;31(8):1537-1549. doi: 10.3201/eid3108.241419. Epub 2025 Jul 1. Emerg Infect Dis. 2025. PMID: 40592354 Free PMC article.
-
Vaccine Based on Recombinant Fusion Protein Combining Hepatitis B Virus PreS with SARS-CoV-2 Wild-Type- and Omicron-Derived Receptor Binding Domain Strongly Induces Omicron-Neutralizing Antibodies in a Murine Model.Vaccines (Basel). 2024 Feb 23;12(3):229. doi: 10.3390/vaccines12030229. Vaccines (Basel). 2024. PMID: 38543863 Free PMC article.
-
Avidity maturation of humoral response following primary and booster doses of BNT162b2 mRNA vaccine among nursing home residents and healthcare workers.Geroscience. 2024 Dec;46(6):6183-6194. doi: 10.1007/s11357-024-01215-y. Epub 2024 May 25. Geroscience. 2024. PMID: 38789833 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Miscellaneous
