

An Updated Systematic Review and Meta-analysis of the Impact of Graduated Compression Stockings in Addition to Pharmacological Thromboprophylaxis for Prevention of Venous Thromboembolism in Surgical Inpatients
- PMID: 37753655
- PMCID: PMC10727201
- DOI: 10.1097/SLA.0000000000006096
An Updated Systematic Review and Meta-analysis of the Impact of Graduated Compression Stockings in Addition to Pharmacological Thromboprophylaxis for Prevention of Venous Thromboembolism in Surgical Inpatients
Abstract
Objective: To compare the rate of venous thromboembolism (VTE) in surgical inpatients with pharmacological thromboprophylaxis and additional graduated compression stockings (GCSs) versus pharmacological thromboprophylaxis alone.
Background: Surgical inpatients have elevated VTE risk; recent studies cast doubt on whether GCS confers additional protection against VTE, compared with pharmacological thromboprophylaxis alone.
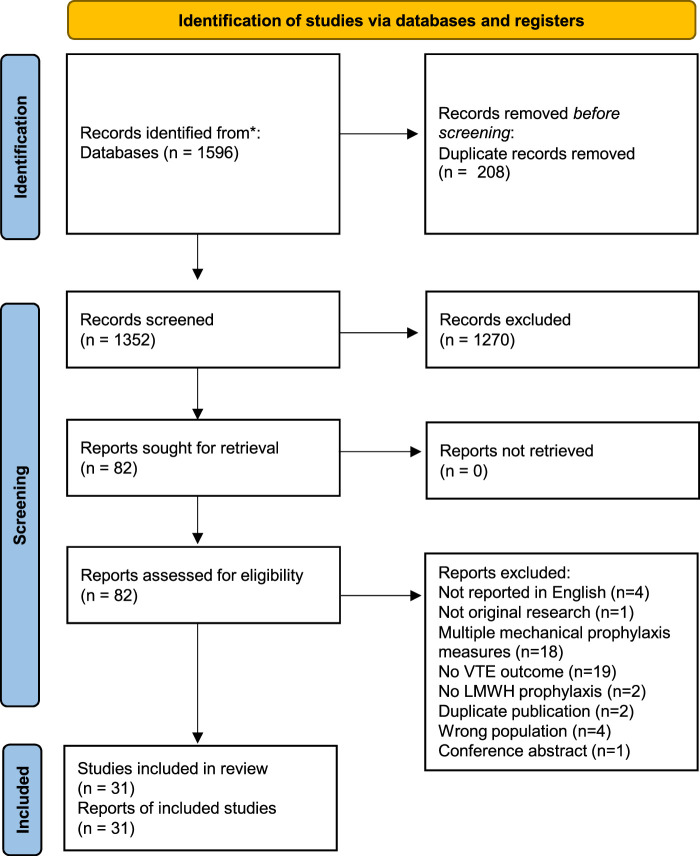
Methods: The review followed "Preferred Reporting Items for Systematic Reviews and Meta-analyses" guidelines using a registered protocol (CRD42017062655). The MEDLINE and Embase databases were searched up to November 2022. Randomized trials reporting VTE rate after surgical procedures, utilizing pharmacological thromboprophylaxis, with or without GCS, were included. The rates of deep venous thrombosis (DVT), pulmonary embolism, and VTE-related mortality were pooled through fixed and random effects.
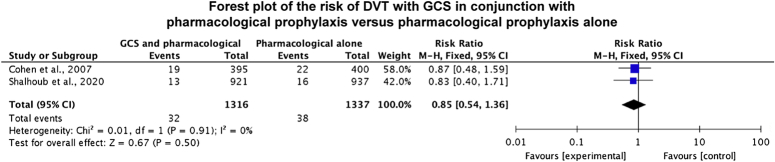
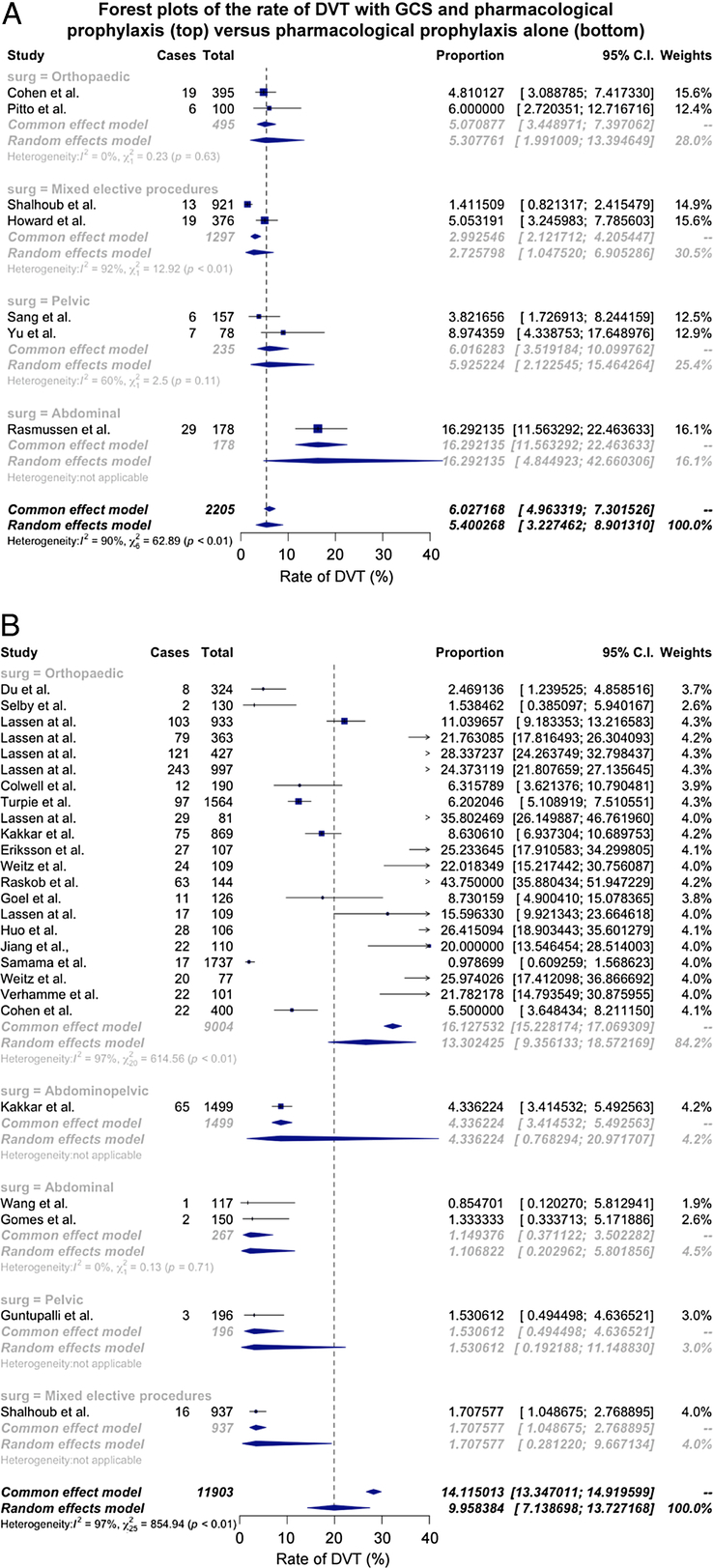
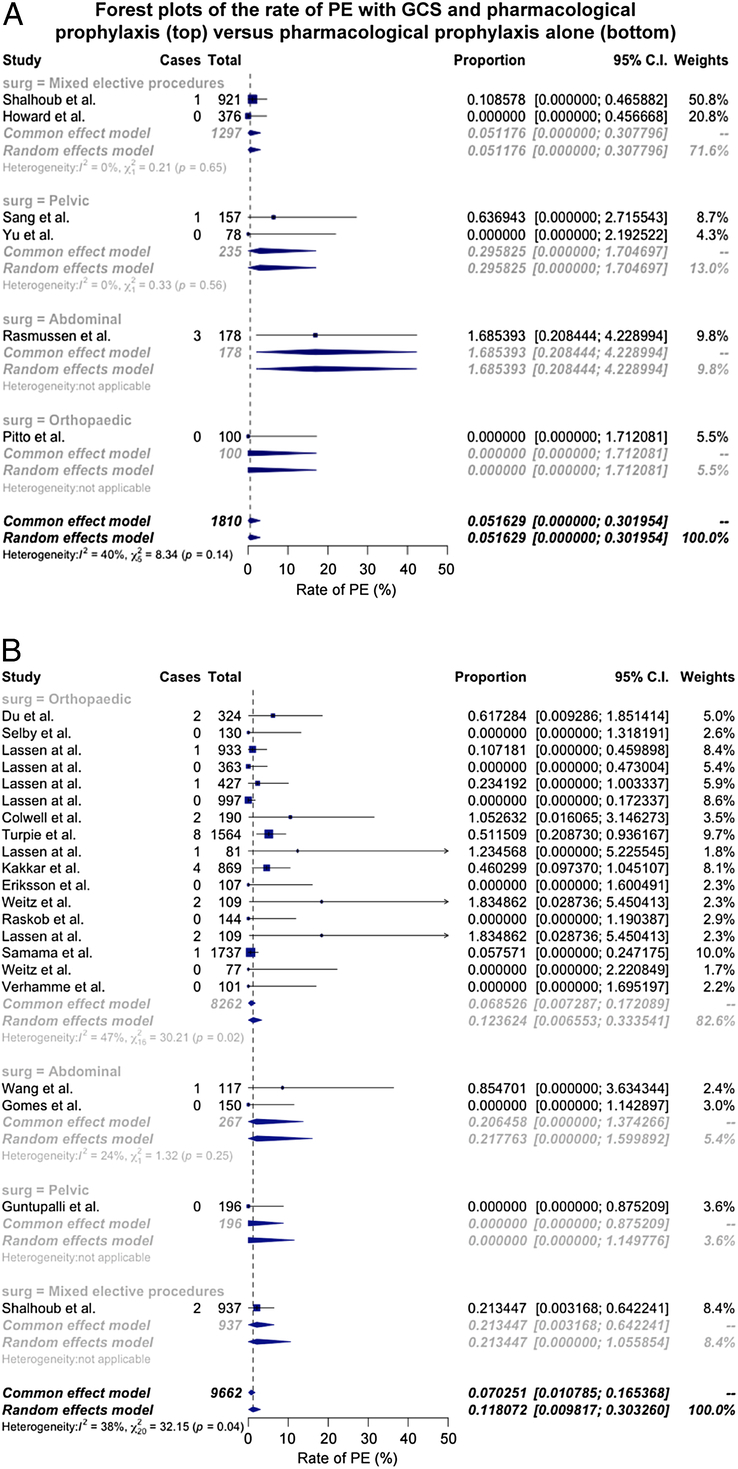
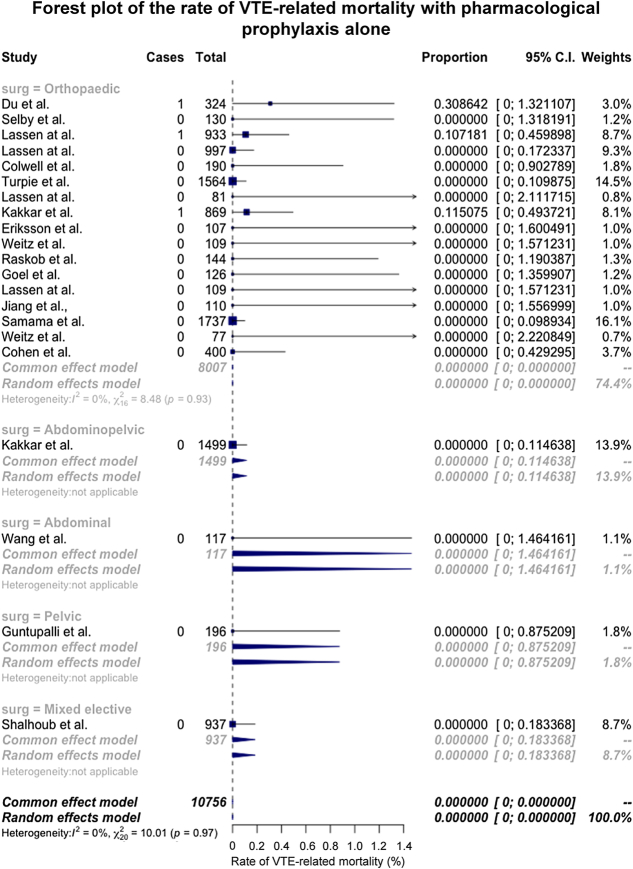
Results: In a head-to-head meta-analysis, the risk of DVT for GCS and pharmacological thromboprophylaxis was 0.85 (95% CI: 0.54-1.36) versus for pharmacological thromboprophylaxis alone (2 studies, 70 events, 2653 participants). The risk of DVT in pooled trial arms for GCS and pharmacological thromboprophylaxis was 0.54 (95% CI: 0.23-1.25) versus pharmacological thromboprophylaxis alone (33 trial arms, 1228 events, 14,108 participants). The risk of pulmonary embolism for GCS and pharmacological prophylaxis versus pharmacological prophylaxis alone was 0.71 (95% CI: 0.0-30.0) (27 trial arms, 32 events, 11,472 participants). There were no between-group differences in VTE-related mortality (27 trial arms, 3 events, 12,982 participants).
Conclusions: Evidence from head-to-head meta-analysis and pooled trial arms demonstrates no additional benefit for GCS in preventing VTE and VTE-related mortality. GCS confer a risk of skin complications and an economic burden; current evidence does not support their use for surgical inpatients.
Copyright © 2023 The Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
A.H.D. is supported by an NIHR Senior Investigator award. The remaining authors report no conflicts of interest.
Figures
References
-
- Cohen AT, Agnelli G, Anderson FA, et al. . Venous thromboembolism (VTE) in Europe. The number of VTE events and associated morbidity and mortality. Thromb Haemost. 2007;98:756–764. - PubMed
-
- Agnelli G. Prevention of venous thromboembolism in surgical patients. Circulation. 2004;110(suppl 1):IV4–IV12. - PubMed
-
- Cohen AT, Tapson VF, Bergmann JF, et al. . Venous thromboembolism risk and prophylaxis in the acute hospital care setting (ENDORSE study): a multinational cross-sectional study. Lancet. 2008;371:387–394. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
