

Death after High-Dose rAAV9 Gene Therapy in a Patient with Duchenne's Muscular Dystrophy
- PMID: 37754285
- PMCID: PMC11288170
- DOI: 10.1056/NEJMoa2307798
Death after High-Dose rAAV9 Gene Therapy in a Patient with Duchenne's Muscular Dystrophy
Abstract
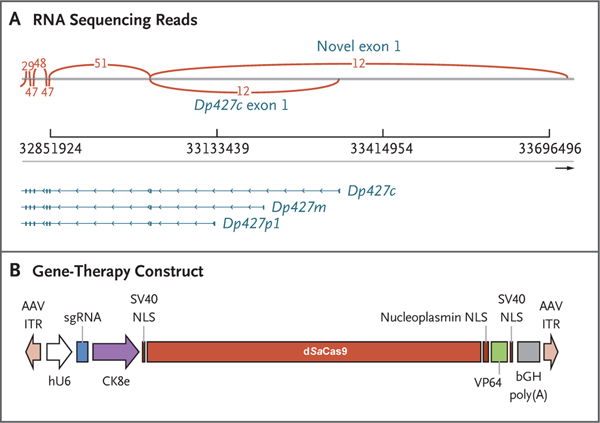
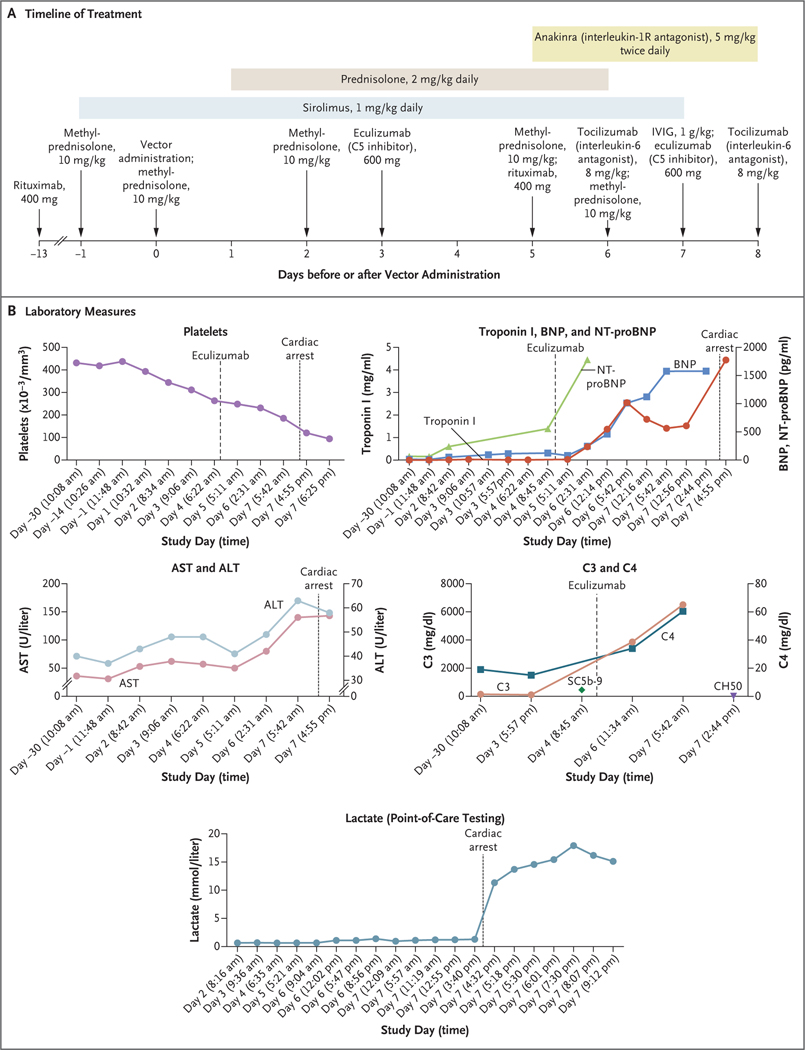
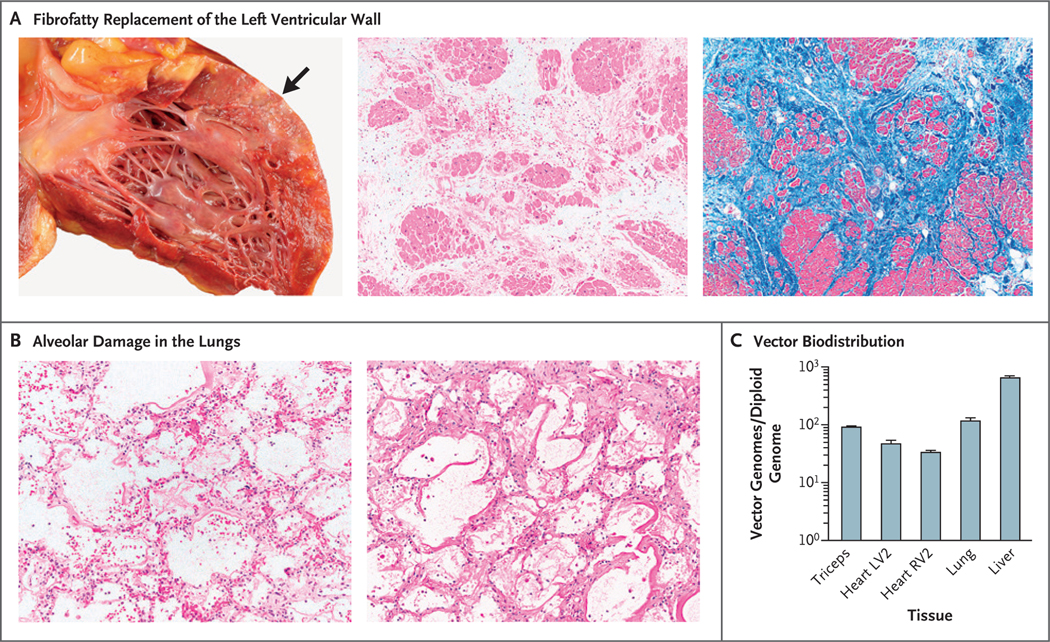
We treated a 27-year-old patient with Duchenne's muscular dystrophy (DMD) with recombinant adeno-associated virus (rAAV) serotype 9 containing dSaCas9 (i.e., "dead" Staphylococcus aureus Cas9, in which the Cas9 nuclease activity has been inactivated) fused to VP64; this transgene was designed to up-regulate cortical dystrophin as a custom CRISPR-transactivator therapy. The dose of rAAV used was 1×1014 vector genomes per kilogram of body weight. Mild cardiac dysfunction and pericardial effusion developed, followed by acute respiratory distress syndrome (ARDS) and cardiac arrest 6 days after transgene treatment; the patient died 2 days later. A postmortem examination showed severe diffuse alveolar damage. Expression of transgene in the liver was minimal, and there was no evidence of AAV serotype 9 antibodies or effector T-cell reactivity in the organs. These findings indicate that an innate immune reaction caused ARDS in a patient with advanced DMD treated with high-dose rAAV gene therapy. (Funded by Cure Rare Disease.).
Copyright © 2023 Massachusetts Medical Society.
Figures
Comment in
-
Death after High-Dose rAAV9 Gene Therapy in a Patient with Duchenne's Muscular Dystrophy.N Engl J Med. 2023 Dec 7;389(23):2210-2211. doi: 10.1056/NEJMc2312288. N Engl J Med. 2023. PMID: 38055267 No abstract available.
-
Death after High-Dose rAAV9 Gene Therapy in a Patient with Duchenne's Muscular Dystrophy.N Engl J Med. 2023 Dec 7;389(23):2211. doi: 10.1056/NEJMc2312288. N Engl J Med. 2023. PMID: 38055268 No abstract available.
-
Death after High-Dose rAAV9 Gene Therapy in a Patient with Duchenne's Muscular Dystrophy. Reply.N Engl J Med. 2023 Dec 7;389(23):2211. doi: 10.1056/NEJMc2312288. N Engl J Med. 2023. PMID: 38055269 No abstract available.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical