

ST-Segment Elevation: An Unexpected Culprit
- PMID: 37754803
- PMCID: PMC10532326
- DOI: 10.3390/jcdd10090374
ST-Segment Elevation: An Unexpected Culprit
Abstract
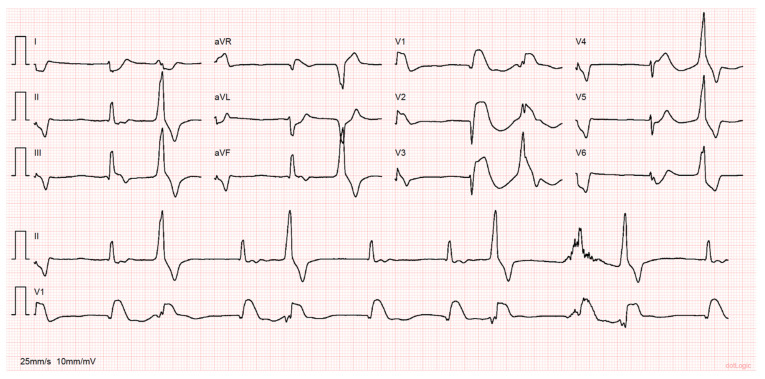
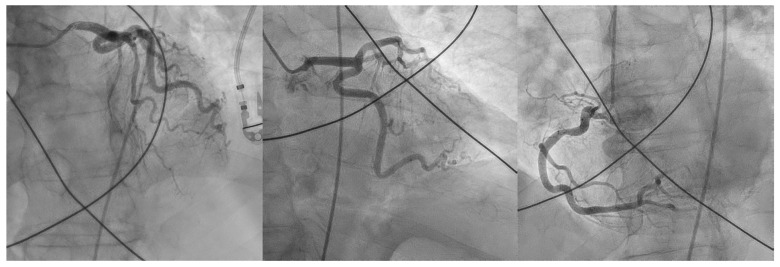
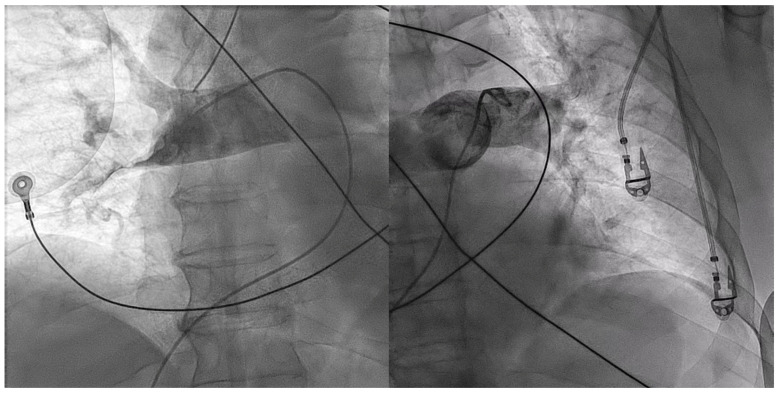
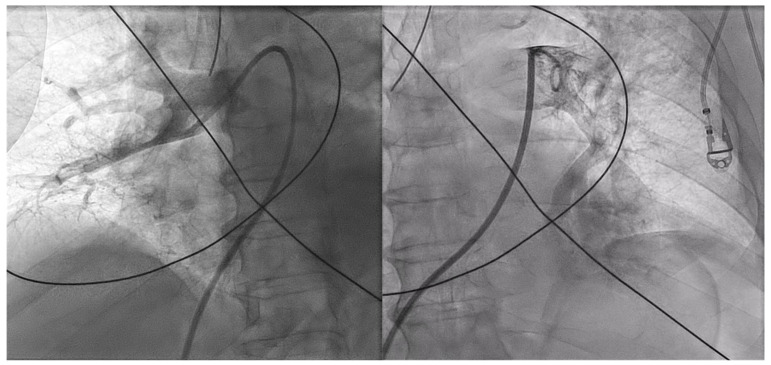
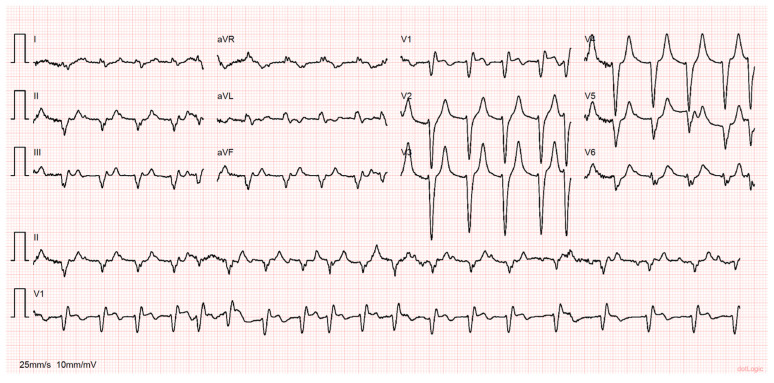
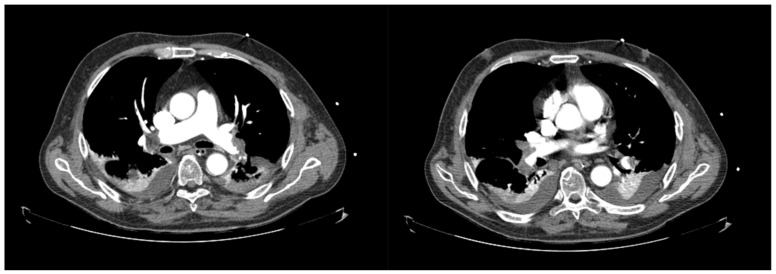
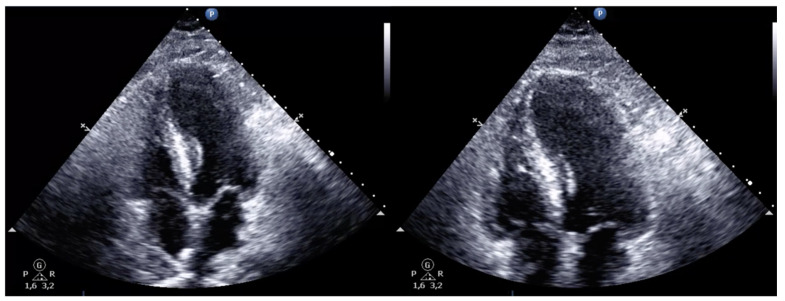
The clinical presentation of pulmonary embolism (PE) and acute coronary syndrome can be similar. We report a case of a patient presenting with antero-septal ST-segment elevation after cardiac arrest, found to have acute-PE-mimicking ST-segment elevation myocardial infarction (STEMI), treated with aspiration thrombectomy and catheter-directed thrombolysis (CDT). A 78-year-old man was admitted with dyspnea, chest pain and tachycardia. During evaluation, cardiac arrest in pulseless electrical activity was documented. Advanced life support was started immediately. ECG post-ROSC revealed ST-segment elevation in V1-V4 and aVR. Echocardiography showed normal left ventricular function but right ventricular (RV) dilation and severe dysfunction. The patient was in shock and was promptly referred to cardiac catheterization that excluded significant CAD. Due to the discordant ECG and echocardiogram findings, acute PE was suspected, and immediate invasive pulmonary angiography revealed bilateral massive pulmonary embolism. Successful aspiration thrombectomy was performed followed by local alteplase infusion. At the end of the procedure, mPAP was reduced and blood pressure normalized allowing withdrawal of vasopressor support. Twenty-four-hour echocardiographic reassessment showed normal-sized cardiac chambers with preserved biventricular systolic function. Bedside echocardiography in patients with ST-segment elevation post-ROSC is instrumental in raising the suspicion of acute PE. In the absence of a culprit coronary lesion, prompt pulmonary angiography should be considered if immediately feasible. In these cases, CDT and aspiration in high-risk acute PE seem safe and effective in relieving obstructive shock and restoring hemodynamics.
Keywords: ST-segment; acute pulmonary embolism; aspiration thrombectomy; catheter-directed therapy; intervention cardiology; thrombolysis.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
ST-segment elevation in V1-V4 in acute pulmonary embolism: a case presentation and review of literature.Eur Heart J Acute Cardiovasc Care. 2016 Dec;5(8):579-586. doi: 10.1177/2048872615604273. Epub 2015 Sep 15. Eur Heart J Acute Cardiovasc Care. 2016. PMID: 26373811 Review.
-
The Crucial Role of Bedside Echocardiography and Clinical Suspicion in Diagnosing Pulmonary Embolism With ST Elevation on ECG, Initially Misdiagnosed as ST-Segment Elevation Myocardial Infarction (STEMI).Cureus. 2024 Dec 26;16(12):e76417. doi: 10.7759/cureus.76417. eCollection 2024 Dec. Cureus. 2024. PMID: 39872588 Free PMC article.
-
Massive pulmonary embolism with ST-segment elevation mimicking an isolated right ventricular myocardial infarction in a patient with COVID-19 pneumonia: Case report.Ann Med Surg (Lond). 2022 Dec;84:104943. doi: 10.1016/j.amsu.2022.104943. Epub 2022 Nov 17. Ann Med Surg (Lond). 2022. PMID: 36415681 Free PMC article.
-
Catheter-directed thrombolysis versus suction thrombectomy in the management of acute pulmonary embolism.J Vasc Surg Venous Lymphat Disord. 2019 Sep;7(5):623-628. doi: 10.1016/j.jvsv.2018.10.025. Epub 2019 Mar 20. J Vasc Surg Venous Lymphat Disord. 2019. PMID: 30902560
-
Case report and systematic review of pulmonary embolism mimicking ST-elevation myocardial infarction.Vascular. 2019 Feb;27(1):90-97. doi: 10.1177/1708538118791917. Epub 2018 Jul 30. Vascular. 2019. PMID: 30056785
Cited by
-
ST Elevation in aVR: An Atypical Presentation of Pulmonary Embolism.Clin Case Rep. 2025 Jul 29;13(8):e70671. doi: 10.1002/ccr3.70671. eCollection 2025 Aug. Clin Case Rep. 2025. PMID: 40741114 Free PMC article.
-
Pulmonary embolism secondary to acute anterior ST-elevation myocardial infarction: a case report.World J Emerg Med. 2024;15(2):139-141. doi: 10.5847/wjem.j.1920-8642.2024.017. World J Emerg Med. 2024. PMID: 38476537 Free PMC article. No abstract available.
References
-
- Pollack C.V., Schreiber D., Goldhaber S.Z., Slattery D., Fanikos J., O’Neil B.J., Thompson J.R., Hiestand B., Briese B.A., Pendleton R.C., et al. Clinical characteristics, management, and outcomes of patients diagnosed with acute pulmonary embolism in the emergency department: Initial report of EMPEROR (Multicenter Emergency Medicine Pulmonary Embolism in the Real World Registry) J. Am. Coll. Cardiol. 2011;57:700–706. doi: 10.1016/j.jacc.2010.05.071. - DOI - PubMed
-
- Konstantinides S.V., Meyer G., Becattini C., Bueno H., Geersing G.J., Harjola V.-P., Huisman M.V., Humbert M., Jennings C.S., Jiménez D., et al. 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS) Eur. Heart J. 2020;41:543–603. doi: 10.1093/eurheartj/ehz405. - DOI - PubMed
-
- Ibanez B., James S., Agewall S., Antunes M.J., Bucciarelli-Ducci C., Bueno H., Caforio A.L.P., Crea F., Goudevenos J.A., Halvorsen S., et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC) Eur. Heart J. 2018;39:119–177. doi: 10.1093/eurheartj/ehx393. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
