

Single-session visuospatial task procedure to prevent childbirth-related posttraumatic stress disorder: a multicentre double-blind randomised controlled trial
- PMID: 37759037
- PMCID: PMC10730415
- DOI: 10.1038/s41380-023-02275-w
Single-session visuospatial task procedure to prevent childbirth-related posttraumatic stress disorder: a multicentre double-blind randomised controlled trial
Abstract
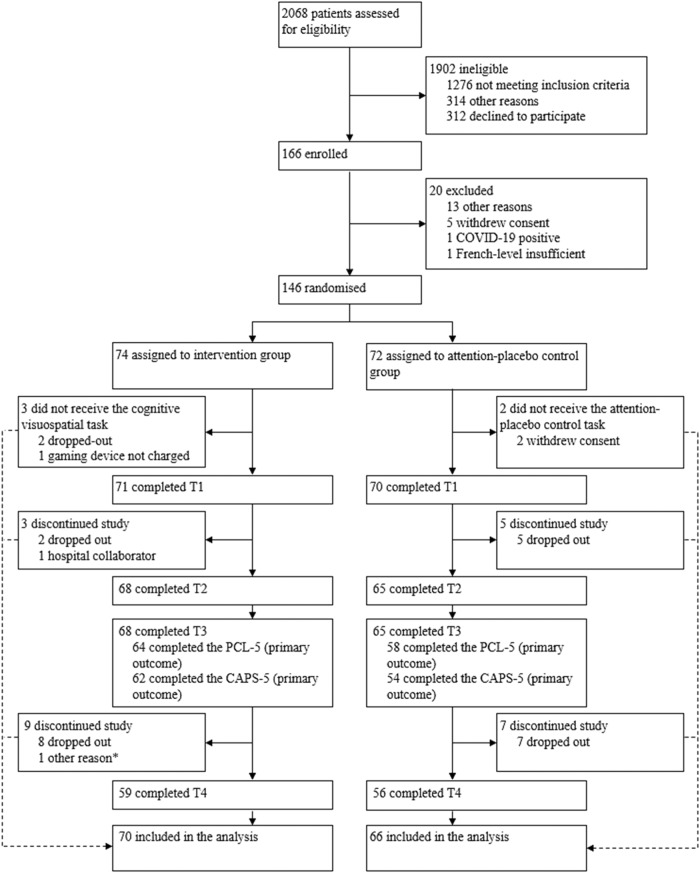
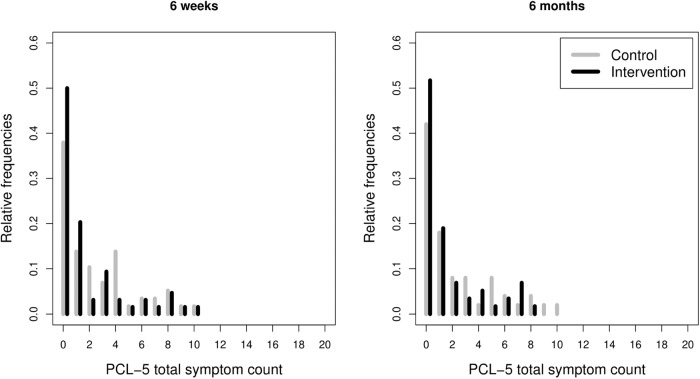
Preventive evidence-based interventions for childbirth-related posttraumatic stress disorder (CB-PTSD) are lacking. Yet, 18.5% of women develop CB-PTSD symptoms following an unplanned caesarean section (UCS). This two-arm, multicentre, double-blind superiority trial tested the efficacy of an early single-session intervention including a visuospatial task on the prevention of maternal CB-PTSD symptoms. The intervention was delivered by trained maternity clinicians. Shortly after UCS, women were included if they gave birth to a live baby, provided consent, and perceived their childbirth as traumatic. Participants were randomly assigned to the intervention or attention-placebo group (allocation ratio 1:1). Assessments were done at birth, six weeks, and six months postpartum. Group differences in maternal CB-PTSD symptoms at six weeks (primary outcomes) and six months postpartum (secondary outcomes) were assessed with the self-report PTSD Checklist for DSM-5 (PCL-5) and by blinded research assessors with the Clinician-administered PTSD scale for DSM-5 (CAPS-5). Analysis was by intention-to-treat. The trial was prospectively registered (ClinicalTrials.gov, NCT03576586). Of the 2068 women assessed for eligibility, 166 were eligible and 146 were randomly assigned to the intervention (n = 74) or attention-placebo control group (n = 72). For the PCL-5, at six weeks, a marginally significant intervention effect was found on the total PCL-5 PTSD symptom count (β = -0.43, S.E. = 0.23, z = -1.88, p < 0.06), and on the intrusions (β = -0.73, S.E. = 0.38, z = -1.94, p < 0.0525) and arousal (β = -0.55, S.E. = 0.29, z = -1.92, p < 0.0552) clusters. At six months, a significant intervention effect on the total PCL-5 PTSD symptom count (β = -0.65, S.E. = 0.32, z = -2.04, p = 0.041, 95%CI[-1.27, -0.03]), on alterations in cognition and mood (β = -0.85, S.E. = 0.27, z = -3.15, p = 0.0016) and arousal (β = -0.56, S.E. = 0.26, z = -2.19, p < 0.0289, 95%CI[-1.07, -0.06]) clusters appeared. No group differences on the CAPS-5 emerged. Results provide evidence that this brief, single-session intervention carried out by trained clinicians can prevent the development of CB-PTSD symptoms up to six months postpartum.
© 2023. The Author(s).
Conflict of interest statement
AH is a management committee member of COST Action CA18211. EAH is on the Board of Trustees of the MQ Foundation. EAH has developed an imagery-competing task intervention for intrusive memories, and training in using it (ANEMONE™). EAH receives book royalties from Guildford Press and Oxford University Press and receives occasional honoraria for conference keynotes and clinical workshops. EAH receives funding from The Wellcome Trust (223016/Z/21/Z), Swedish Research Council (2020–00873), OAK foundation (OCAY-18-442), AFA Försäkring (200,342), The Lupina Foundation and Rannís The Icelandic Research Fund. Other authors declare no competing interests. The funder of the study, the Swiss National Science Foundation, had no role in the study design, data collection, data analysis, data interpretation, report writing, or the decision to submit the paper.
Figures
References
-
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders (5th ed.). Arlington, VA: American Psychiatric Publishing; 2013.
-
- Heyne C-S, Kazmierczak M, Souday R, Horesh D, den Berg MLV, Weigl T, et al. Prevalence and risk factors of birth-related posttraumatic stress among parents: a comparative systematic review and meta-analysis. Clin Psychol Rev. 2022;94:102157. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
