

Prophylactic platelet transfusion response in critically ill patients: a prospective multicentre observational study
- PMID: 37759268
- PMCID: PMC10537531
- DOI: 10.1186/s13054-023-04650-z
Prophylactic platelet transfusion response in critically ill patients: a prospective multicentre observational study
Abstract
Background: Response to prophylactic platelet transfusion is suspected to be inconsistent in critically ill patients questioning how to optimize transfusion practices. This study aimed to describe prophylactic platelet transfusion response, to identify factors associated with a suboptimal response, to analyse the correlation between corrected count increment and platelet count increment and to determine the association between poor platelet transfusion response and clinical outcomes.
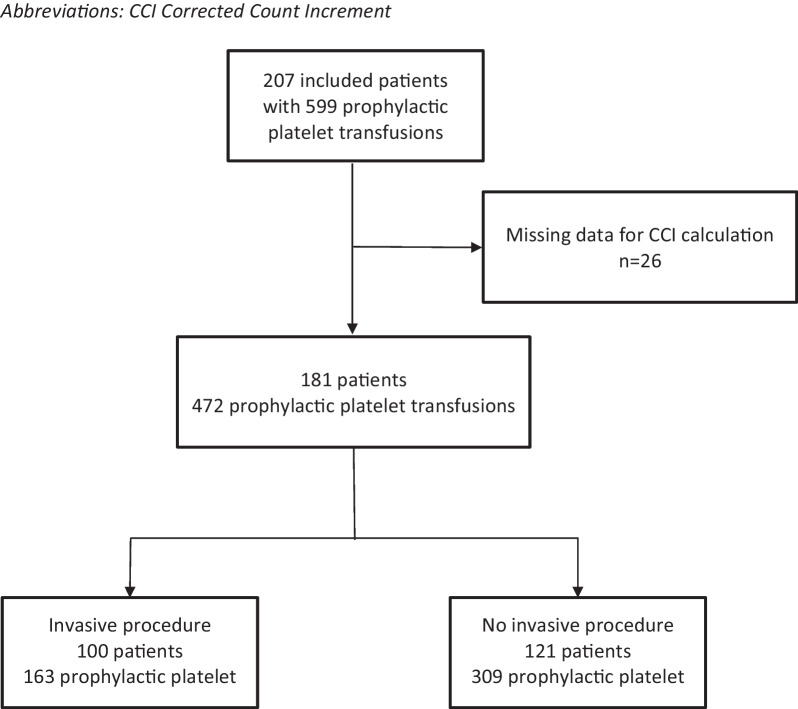
Methods: This prospective multicentre observational study recruited patients who received at least one prophylactic platelet transfusion in one of the nine participating intensive care units for a period up to 16 months. Poor platelet transfusion response was defined as a corrected count increment (CCI) that adjusts for platelet dose and body surface area, less than 7 at 18-24 h after platelet transfusion. Factors associated with poor platelet transfusion response were assessed in a mixed-effect model. Sensitivity analyses were conducted in patients with and without haematology malignancy and chemotherapy.
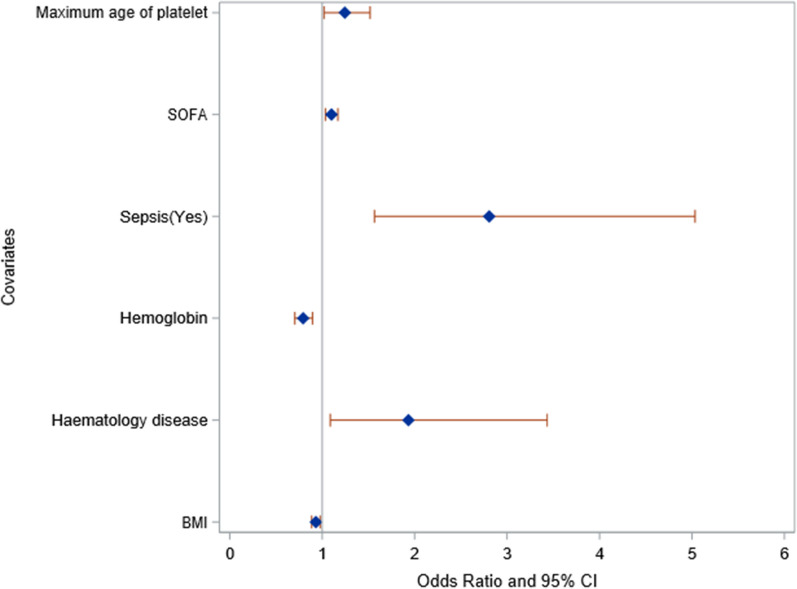
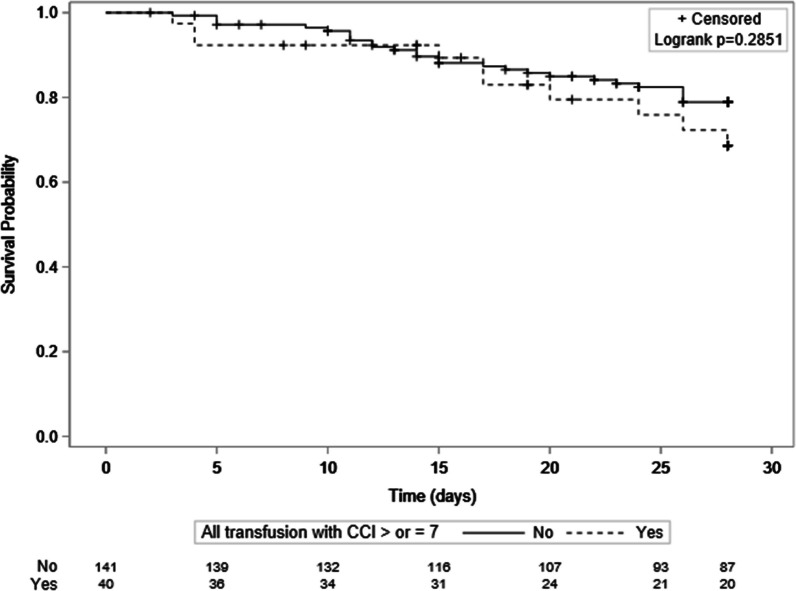
Results: Poor platelet transfusion response occurred in 349 of the 472 (73.9%) prophylactic platelet transfusions and in 141/181 (77.9%) patients. The mixed-effect model identified haemoglobin at ICU admission (odds ratio (OR): 0.79 [95% confidence interval (CI) 0.7-0.89]) and body mass index (BMI) (OR: 0.93 [0.89-0.98]) being positively and independently associated with platelet transfusion response, while a haematological malignancy (OR 1.93 [1.09-3.43]), sepsis as primary ICU admission diagnosis (OR: 2.81 [1.57-5.03]), SOFA score (OR 1.10 [1.03; 1.17]) and maximum storage duration of platelet (OR: 1.24 [1.02-1.52]) were independently associated with a suboptimal platelet increment. Clinical outcomes did not differ between groups, nor the requirement for red blood cells. Poor platelet transfusion response was found in 93.5% of patients with haematology malignancy and chemotherapy.
Conclusions: In this study of critically ill patients, of whom more than half had bone marrow failure, almost three quarters of prophylactic platelet transfusions led to suboptimal platelet increment measured 18 to 24 h following platelet transfusion. Platelet storage duration was the only factor associated with poor platelet response that may be accessible to intervention. Trial registration in October 2017: ClinicalTrials.gov: NCT03325140.
Keywords: Bleeding; Critically ill patient; Platelet transfusion response; Prophylactic transfusion.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Wandt H, Schaefer-Eckart K, Wendelin K, Pilz B, Wilhelm M, Thalheimer M, Mahlknecht U, Ho A, Schaich M, Kramer M, et al. Therapeutic platelet transfusion versus routine prophylactic transfusion in patients with haematological malignancies: an open-label, multicentre, randomised study. Lancet. 2012;380(9850):1309–1316. doi: 10.1016/S0140-6736(12)60689-8. - DOI - PubMed
-
- van Baarle FLF, van de Weerdt EK, van der Velden W, Ruiterkamp RA, Tuinman PR, Ypma PF, van den Bergh WM, Demandt AMP, Kerver ED, Jansen AJG, et al. Platelet transfusion before CVC placement in patients with thrombocytopenia. N Engl J Med. 2023;388(21):1956–1965. doi: 10.1056/NEJMoa2214322. - DOI - PubMed
-
- Vlaar AP, Oczkowski S, de Bruin S, Wijnberge M, Antonelli M, Aubron C, Aries P, Duranteau J, Juffermans NP, Meier J, et al. Transfusion strategies in non-bleeding critically ill adults: a clinical practice guideline from the European Society of Intensive Care Medicine. Intensive Care Med. 2020;46(4):673–696. doi: 10.1007/s00134-019-05884-8. - DOI - PMC - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
