

Cost-Effectiveness Analysis of Risk Factor-Based Lung Cancer Screening Program by Low-Dose Computer Tomography in Current Smokers in China
- PMID: 37760416
- PMCID: PMC10527380
- DOI: 10.3390/cancers15184445
Cost-Effectiveness Analysis of Risk Factor-Based Lung Cancer Screening Program by Low-Dose Computer Tomography in Current Smokers in China
Abstract
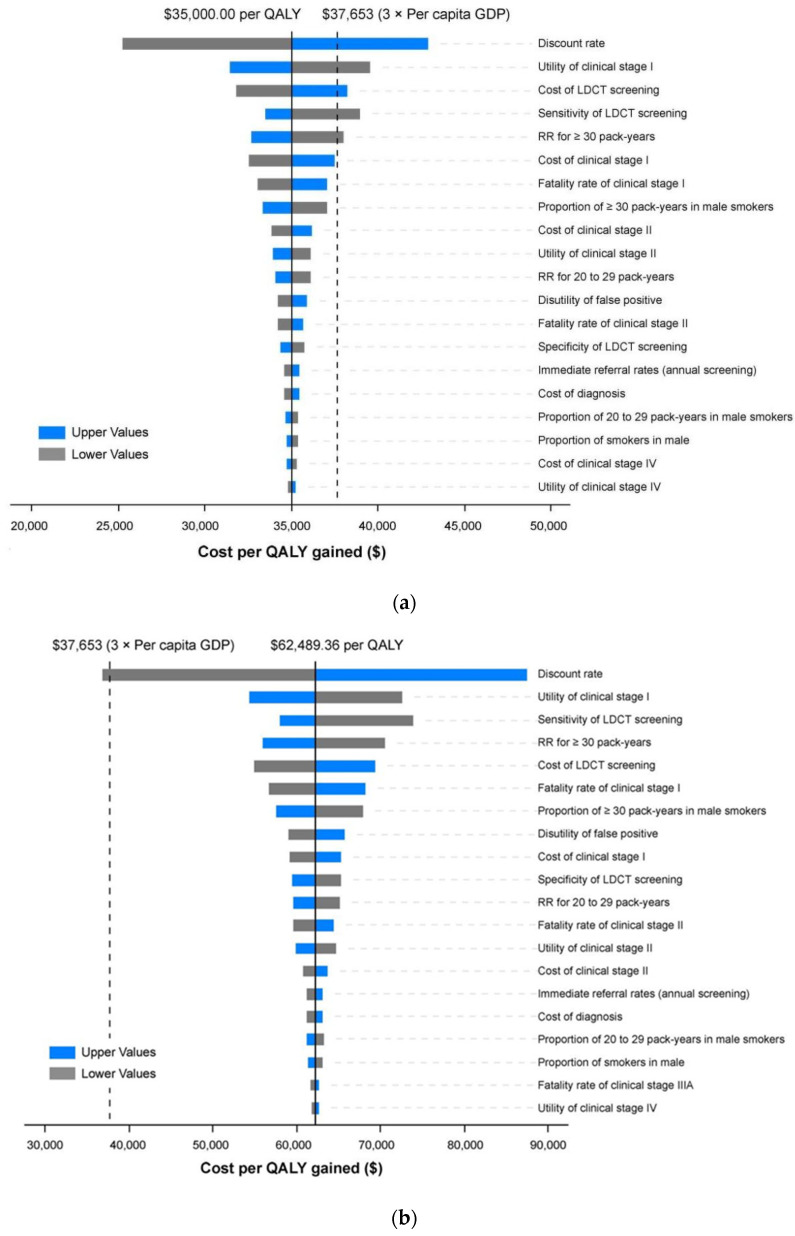
Although the effectiveness of lung cancer screening by low-dose computed tomography (LDCT) could be shown in China, there could be variation in the evidence concerning the economic impact. Our study explores the cost-effectiveness of lung cancer screening and optimizes the best definition of a high-risk population. A Markov model consisting of the natural history and post-diagnosis states was constructed to estimate the costs and quality-adjusted life years (QALYs) of LDCT screening compared with no screening. A total of 36 distinct risk factor-based screening strategies were assessed by incorporating starting ages of 40, 45, 50, 55, 60 and 65 years, stopping ages of 69, 74 and 79 years as well as smoking eligibility criteria. Screening data came from community-based mass screening with LDCT for lung cancer in Guangzhou. Compared with no screening, all screening scenarios led to incremental costs and QALYs. When the willingness-to-pay (WTP) threshold was USD37,653, three times the gross domestic product (GDP) per capita in China, six of nine strategies on the efficiency frontier may be cost-effective. Annual screening between 55 and 79 years of age for those who smoked more than 20 pack-years, which yielded an incremental cost-effectiveness ratio (ICER) of USD35,000.00 per QALY gained, was considered optimal. In sensitivity analyses, the result was stable in most cases. The trends of the results are roughly the same in scenario analyses. According to the WTP threshold of different regions, the optimal screening strategies were annual screening for those who smoked more than 20 pack-years, between 50 and 79 years of age in Zhejiang province, 55-79 years in Guangdong province and 65-74 years in Yunnan province. However, annual screening was unlikely to be cost-effective in Heilongjiang province under our modelling assumptions, indicating that tailored screening policies should be made regionally according to the local epidemiological and economic situation.
Keywords: China; LDCT screening; cost-effectiveness analysis; current smokers; lung cancer.
Conflict of interest statement
The authors declare no conflict of interest.
Figures



Similar articles
-
Cost-effectiveness of low-dose CT screening for non-smokers with a first-degree relative history of lung cancer.BMC Public Health. 2025 May 15;25(1):1783. doi: 10.1186/s12889-025-22977-w. BMC Public Health. 2025. PMID: 40375086 Free PMC article.
-
Cost-effectiveness of risk model-based lung cancer screening in smokers and nonsmokers in China.BMC Med. 2025 May 28;23(1):315. doi: 10.1186/s12916-025-04065-3. BMC Med. 2025. PMID: 40437557 Free PMC article.
-
Cost-effectiveness of Low-Dose Computed Tomography With a Plasma-Based Biomarker for Lung Cancer Screening in China.JAMA Netw Open. 2022 May 2;5(5):e2213634. doi: 10.1001/jamanetworkopen.2022.13634. JAMA Netw Open. 2022. PMID: 35608858 Free PMC article.
-
[Cost-effectiveness of lung cancer screening worldwide: a systematic review].Zhonghua Liu Xing Bing Xue Za Zhi. 2019 Feb 10;40(2):218-226. doi: 10.3760/cma.j.issn.0254-6450.2019.02.018. Zhonghua Liu Xing Bing Xue Za Zhi. 2019. PMID: 30744276 Chinese.
-
Population-Based Screening Using Low-Dose Chest Computed Tomography: A Systematic Review of Health Economic Evaluations.Pharmacoeconomics. 2023 Apr;41(4):395-411. doi: 10.1007/s40273-022-01238-3. Epub 2023 Jan 20. Pharmacoeconomics. 2023. PMID: 36670332 Free PMC article.
Cited by
-
Cost-effectiveness of low-dose CT screening for non-smokers with a first-degree relative history of lung cancer.BMC Public Health. 2025 May 15;25(1):1783. doi: 10.1186/s12889-025-22977-w. BMC Public Health. 2025. PMID: 40375086 Free PMC article.
-
Cost-Effectiveness of Low-Dose Computed Tomography Screenings for Lung Cancer in High-Risk Populations: A Markov Model.World J Oncol. 2024 Aug;15(4):550-561. doi: 10.14740/wjon1882. Epub 2024 Jul 5. World J Oncol. 2024. PMID: 38993243 Free PMC article.
-
Diameter thresholds for pure ground-glass pulmonary nodules at low-dose CT screening: Chinese experience.Thorax. 2025 Jan 17;80(2):76-85. doi: 10.1136/thorax-2024-221642. Thorax. 2025. PMID: 39689940 Free PMC article.
References
-
- Global Burden of Disease Cancer Collaboration Global, Regional, and National Cancer Incidence, Mortality, Years of Life Lost, Years Lived With Disability, and Disability-Adjusted Life-Years for 29 Cancer Groups, 1990 to 2016: A Systematic Analysis for the Global Burden of Disease Study. JAMA Oncol. 2018;4:1553–1568. doi: 10.1001/jamaoncol.2018.2706. - DOI - PMC - PubMed
-
- Sun K., Zheng R., Zeng H., Zhang S., Zou X., Gu X., Xia C., Yang Z., Li H., Chen W., et al. The incidence and mortality of lung cancer in China, 2014. Chin. J. Oncol. 2018;40:805–811. - PubMed
-
- Zheng R., Zhang S., Sun K., Chen R., Wang S., Li L., Zeng H., Wei W., He J. Cancer statistics in China, 2016. Chin. J. Oncol. 2023;45:212–220. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
