

Therapeutic Potential of Chlorhexidine-Loaded Calcium Hydroxide-Based Intracanal Medications in Endo-Periodontal Lesions: An Ex Vivo and In Vitro Study
- PMID: 37760713
- PMCID: PMC10525524
- DOI: 10.3390/antibiotics12091416
Therapeutic Potential of Chlorhexidine-Loaded Calcium Hydroxide-Based Intracanal Medications in Endo-Periodontal Lesions: An Ex Vivo and In Vitro Study
Abstract
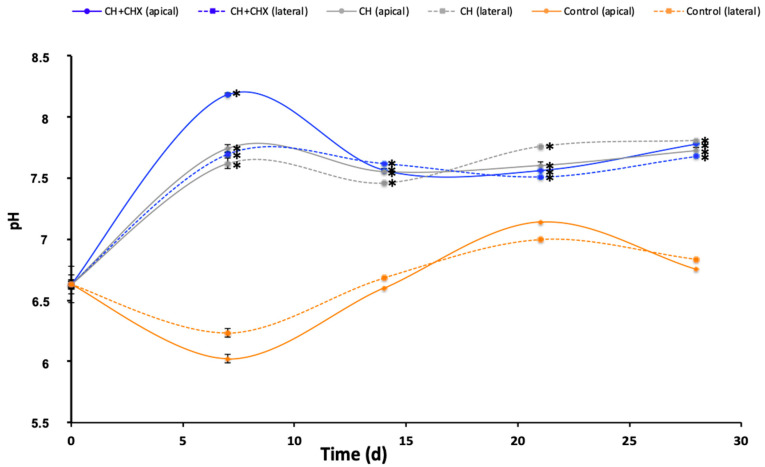
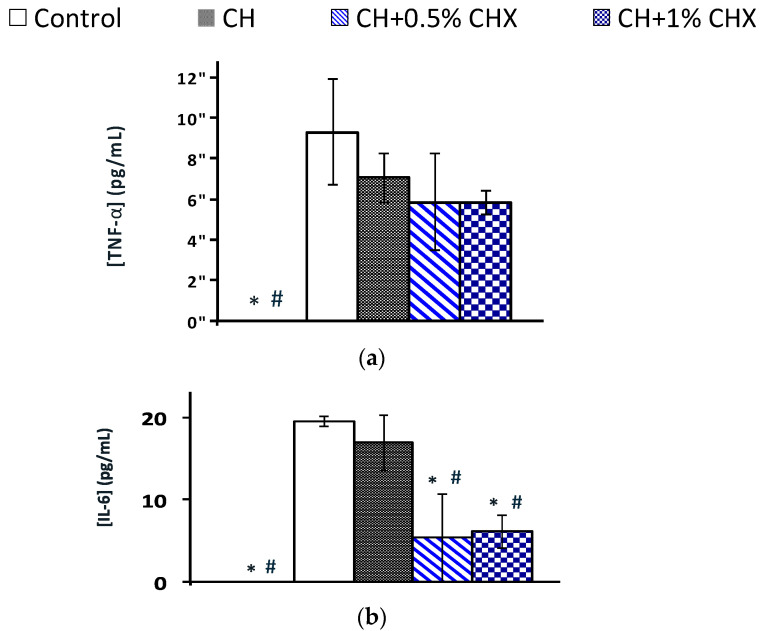
Endo-periodontal lesions are challenging clinical situations where both the supporting tissues and the root canal of the same tooth are infected. In the present study, chlorhexidine (CHX)-loaded calcium hydroxide (CH) pastes were used as intracanal medications (ICMs). They were prepared and tested on pathogens found in both the root canal and the periodontal pocket. Exposure to 0.5% and 1% CHX-loaded ICMs decreased the growth of Porphyromonas gingivalis and was effective in eradicating or inhibiting an Enterococcus faecalis biofilm. CH was injected into the root canal of extracted human teeth immersed in deionized water. CHX-loaded ICMs resulted in the transradicular diffusion of active components outside the tooth through the apex and the lateral dentinal tubules, as shown by the release of CHX (from 3.99 µg/mL to 51.28 µg/mL) and changes in pH (from 6.63 to 8.18) and calcium concentrations (from 2.42 ppm to 14.67 ppm) after 7 days. The 0.5% CHX-loaded ICM was non-toxic and reduced the release of IL-6 by periodontal cells stimulated by P. gingivalis lipopolysaccharides. Results indicate that the root canal may serve as a reservoir for periodontal drug delivery and that CHX-based ICMs can be an adjuvant for the control of infections and inflammation in endo-periodontal lesions.
Keywords: endo-periodontal lesions; intracanal medication; ion release; local drug delivery; periodontal cells.
Conflict of interest statement
The authors declare no conflict of interest.
Figures







Similar articles
-
Antibacterial Efficacy of Pastes Against E Faecalis in Primary Root Dentin: A Confocal Microscope Study.J Clin Pediatr Dent. 2015 Spring;39(3):247-54. doi: 10.17796/1053-4628-39.3.247. J Clin Pediatr Dent. 2015. PMID: 26208070
-
Effectiveness of chitosan-propolis nanoparticle against Enterococcus faecalis biofilms in the root canal.BMC Oral Health. 2020 Nov 25;20(1):339. doi: 10.1186/s12903-020-01330-0. BMC Oral Health. 2020. PMID: 33238961 Free PMC article.
-
Antimicrobial Activity and Physicochemical Properties of Calcium Hydroxide Pastes Used as Intracanal Medication.J Endod. 2016 Dec;42(12):1822-1828. doi: 10.1016/j.joen.2016.08.017. Epub 2016 Oct 21. J Endod. 2016. PMID: 27776884
-
Residual antibacterial effect of calcium hydroxide combined with chlorhexidine gel as an intracanal medicament.Indian J Dent Res. 2020 Nov-Dec;31(6):846-851. doi: 10.4103/ijdr.IJDR_359_19. Indian J Dent Res. 2020. PMID: 33753652
-
In vitro comparison of the effectiveness of chlorhexidine and two calcium hydroxide formulations on enterococcus faecalis.Iran Endod J. 2008 Summer;3(3):50-6. Epub 2008 Jul 10. Iran Endod J. 2008. PMID: 24146671 Free PMC article.
Cited by
-
Endo-Periodontal Lesions in Endodontically Treated Teeth with Periapical Pathology.Diagnostics (Basel). 2025 Jun 30;15(13):1663. doi: 10.3390/diagnostics15131663. Diagnostics (Basel). 2025. PMID: 40647662 Free PMC article.
References
-
- Papapanou P.N., Sanz M., Buduneli N., Dietrich T., Feres M., Fine D.H., Flemmig T.F., Garcia R., Giannobile W.V., Graziani F., et al. Periodontitis: Consensus report of workgroup 2 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Clin. Periodontol. 2018;45:S162–S170. doi: 10.1111/jcpe.12946. - DOI - PubMed
-
- Altaf D.A., Jeelani D.M., Basher D.A. Assessment of prevalence of Endo-perio lesions among patients of known population: An observational study. Int. J. Appl. Dent. Sci. 2019;5:111–113.
-
- Prashaanthi N., Rajasekar A., Shantha Sundari K.K. Prevalence of endo perio lesion-an institutional study. Int. J. Dent. Oral Sci. 2021;8:2858–2862.
-
- Ruetters M., Gehrig H., Kronsteiner D., Schuessler D.L., Kim T.S. Prevalence of endo-perio lesions according to the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Disease in a university hospital. Quintessence Int. 2022;53:134–142. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
