

Distinct Cerebrospinal Fluid Lipid Signature in Patients with Subarachnoid Hemorrhage-Induced Hydrocephalus
- PMID: 37760800
- PMCID: PMC10525923
- DOI: 10.3390/biomedicines11092360
Distinct Cerebrospinal Fluid Lipid Signature in Patients with Subarachnoid Hemorrhage-Induced Hydrocephalus
Abstract
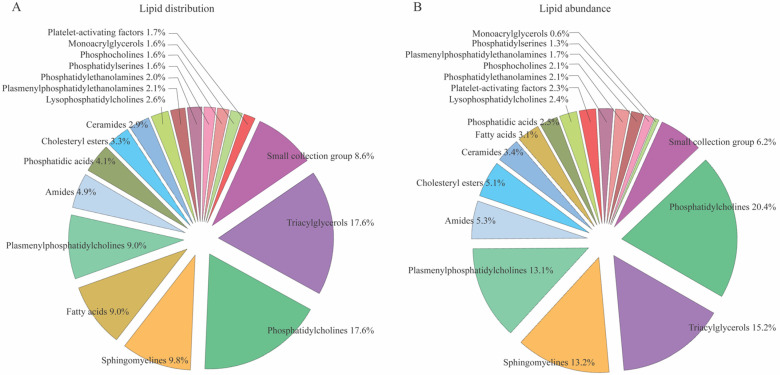
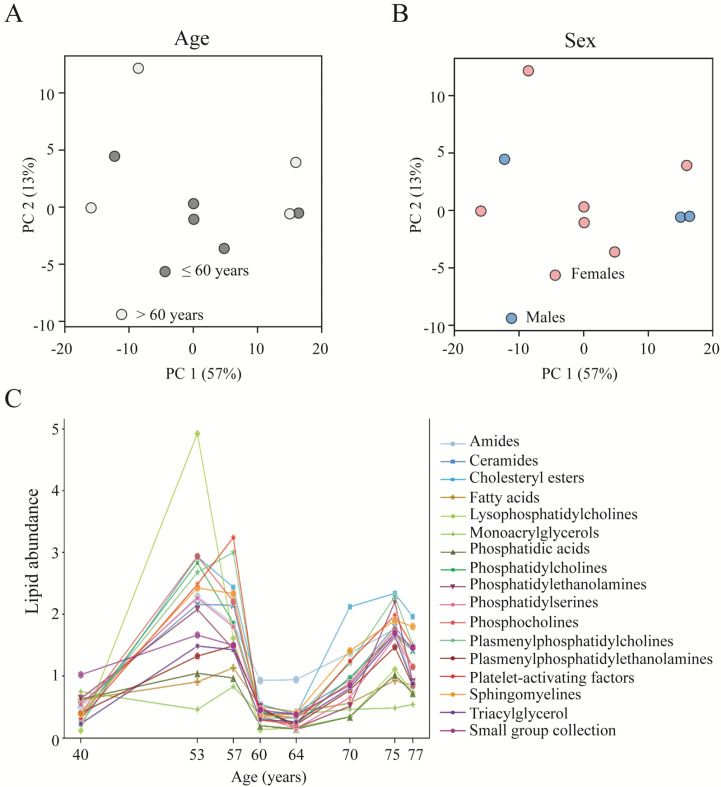
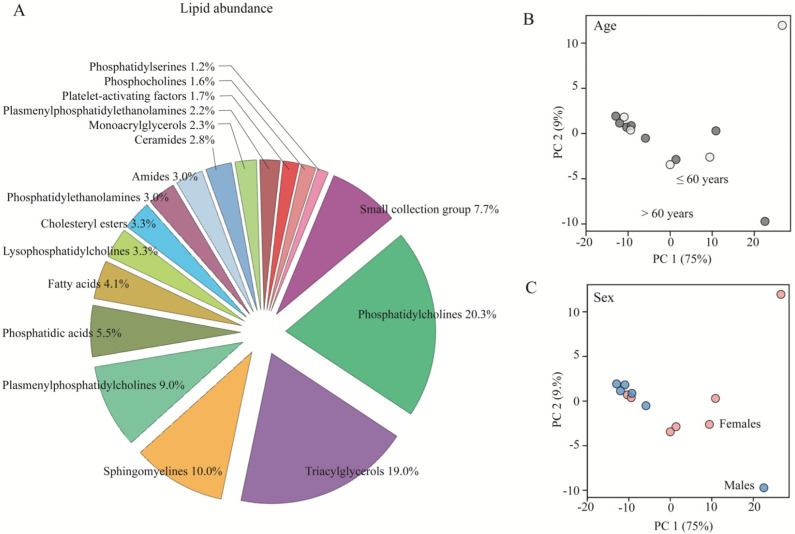
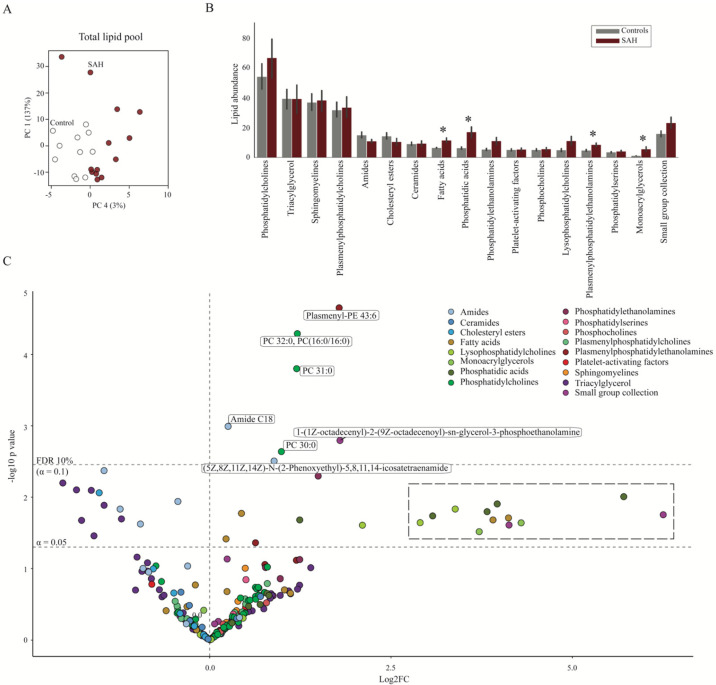
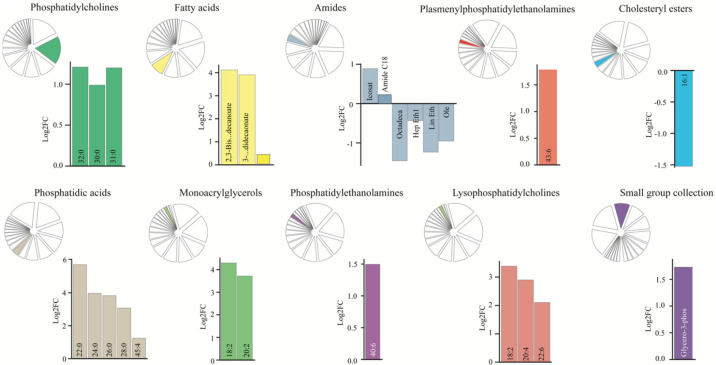
Patients with subarachnoid hemorrhage (SAH) may develop posthemorrhagic hydrocephalus (PHH), which is treated with surgical cerebrospinal fluid (CSF) diversion. This diversion is associated with risk of infection and shunt failure. Biomarkers for PHH etiology, CSF dynamics disturbances, and potentially subsequent shunt dependency are therefore in demand. With the recent demonstration of lipid-mediated CSF hypersecretion contributing to PHH, exploration of the CSF lipid signature in relation to brain pathology is of interest. Despite being a relatively new addition to the omic's landscape, lipidomics are increasingly recognized as a tool for biomarker identification, as they provide a comprehensive overview of lipid profiles in biological systems. We here employ an untargeted mass spectroscopy-based platform and reveal the complete lipid profile of cisternal CSF from healthy control subjects and demonstrate its bimodal fluctuation with age. Various classes of lipids, in addition to select individual lipids, were elevated in the ventricular CSF obtained from patients with SAH during placement of an external ventricular drain. The lipidomic signature of the CSF in the patients with SAH suggests dysregulation of the lipids in the CSF in this patient group. Our data thereby reveal possible biomarkers present in a brain pathology with a hemorrhagic event, some of which could be potential future biomarkers for hypersecretion contributing to ventriculomegaly and thus pharmacological targets for pathologies involving disturbed CSF dynamics.
Keywords: SAH; cerebrospinal fluid; lipidomics; mass spectrometry; posthemorrhagic hydrocephalus.
Conflict of interest statement
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analysis, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Figures
Similar articles
-
Proteomic profile and predictive markers of outcome in patients with subarachnoid hemorrhage.Clin Proteomics. 2024 Jul 23;21(1):51. doi: 10.1186/s12014-024-09493-6. Clin Proteomics. 2024. PMID: 39044147 Free PMC article.
-
Posthemorrhagic hydrocephalus associates with elevated inflammation and CSF hypersecretion via activation of choroidal transporters.Fluids Barriers CNS. 2022 Aug 10;19(1):62. doi: 10.1186/s12987-022-00360-w. Fluids Barriers CNS. 2022. PMID: 35948938 Free PMC article.
-
Posthemorrhagic Hydrocephalus in Patients with Subarachnoid Hemorrhage Occurs Independently of CSF Osmolality.Int J Mol Sci. 2023 Jul 14;24(14):11476. doi: 10.3390/ijms241411476. Int J Mol Sci. 2023. PMID: 37511234 Free PMC article.
-
Post-hemorrhagic hydrocephalus: Recent advances and new therapeutic insights.J Neurol Sci. 2017 Apr 15;375:220-230. doi: 10.1016/j.jns.2017.01.072. Epub 2017 Feb 1. J Neurol Sci. 2017. PMID: 28320134 Review.
-
Is ventricular lavage a novel treatment of neonatal posthemorrhagic hydrocephalus? a meta analysis.Childs Nerv Syst. 2023 Apr;39(4):929-935. doi: 10.1007/s00381-022-05790-3. Epub 2023 Jan 9. Childs Nerv Syst. 2023. PMID: 36622374 Review.
Cited by
-
Proteomic profile and predictive markers of outcome in patients with subarachnoid hemorrhage.Clin Proteomics. 2024 Jul 23;21(1):51. doi: 10.1186/s12014-024-09493-6. Clin Proteomics. 2024. PMID: 39044147 Free PMC article.
-
The Na+,K+,2Cl- Cotransporter, Not Aquaporin 1, Sustains Cerebrospinal Fluid Secretion While Controlling Brain K+ Homeostasis.Adv Sci (Weinh). 2025 Feb;12(6):e2409120. doi: 10.1002/advs.202409120. Epub 2024 Dec 18. Adv Sci (Weinh). 2025. PMID: 39692709 Free PMC article.
-
Metabolomic and lipidomic pathways in aneurysmal subarachnoid hemorrhage.Neurotherapeutics. 2025 Jan;22(1):e00504. doi: 10.1016/j.neurot.2024.e00504. Epub 2024 Dec 19. Neurotherapeutics. 2025. PMID: 39701893 Free PMC article. Review.
-
The CSF lipid profile in patients with probable idiopathic normal pressure hydrocephalus differs from control but does not differ between shunt responders and non-responders.Brain Commun. 2024 Nov 5;6(6):fcae388. doi: 10.1093/braincomms/fcae388. eCollection 2024. Brain Commun. 2024. PMID: 39544703 Free PMC article.
References
-
- Connolly E.S., Jr., Rabinstein A.A., Carhuapoma J.R., Derdeyn C.P., Dion J., Higashida R.T., Hoh B.L., Kirkness C.J., Naidech A.M., Ogilvy C.S., et al. Guidelines for the management of aneurysmal subarachnoid hemorrhage: A guideline for healthcare professionals from the American Heart Association/american Stroke Association. Stroke. 2012;43:1711–1737. doi: 10.1161/STR.0b013e3182587839. - DOI - PubMed
-
- Hoh B.L., Ko N.U., Amin-Hanjani S., Chou S.-Y., Cruz-Flores S., Dangayach N.S., Derdeyn C.P., Du R., Hanggi D., Hetts S.W., et al. 2023 Guideline for the Management of Patients With Aneurysmal Subarachnoid Hemorrhage: A Guideline From the American Heart Association/American Stroke Association. Stroke. 2023;54:e314–e370. doi: 10.1161/STR.0000000000000436. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
