

Neuroendovascular Surgery Applications in Craniocervical Trauma
- PMID: 37760850
- PMCID: PMC10525707
- DOI: 10.3390/biomedicines11092409
Neuroendovascular Surgery Applications in Craniocervical Trauma
Abstract
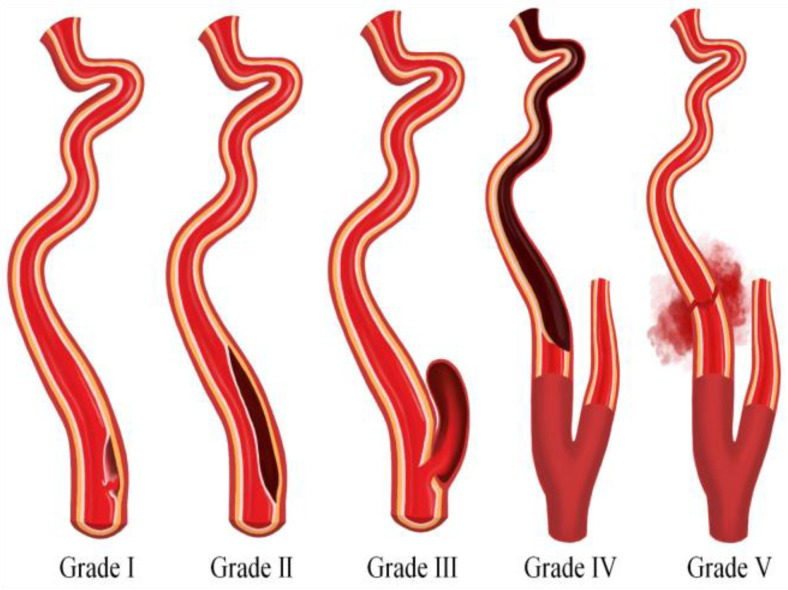
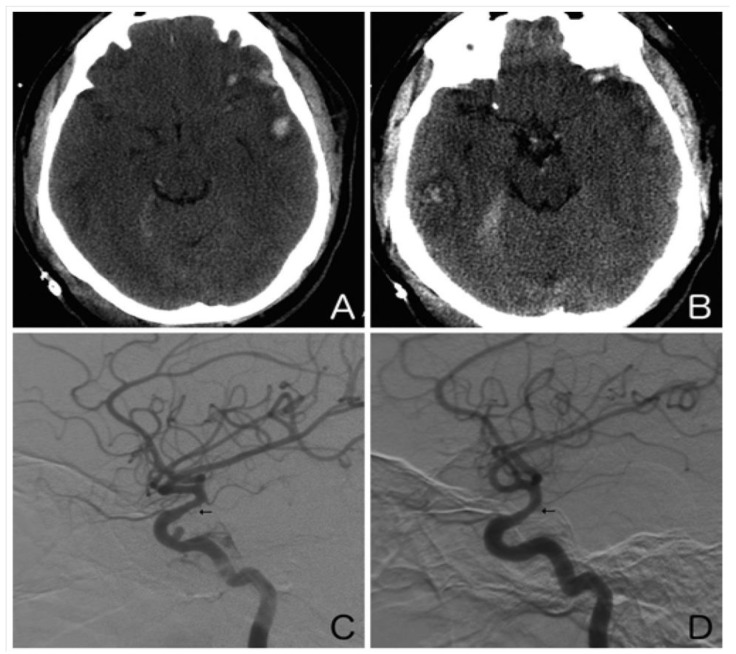
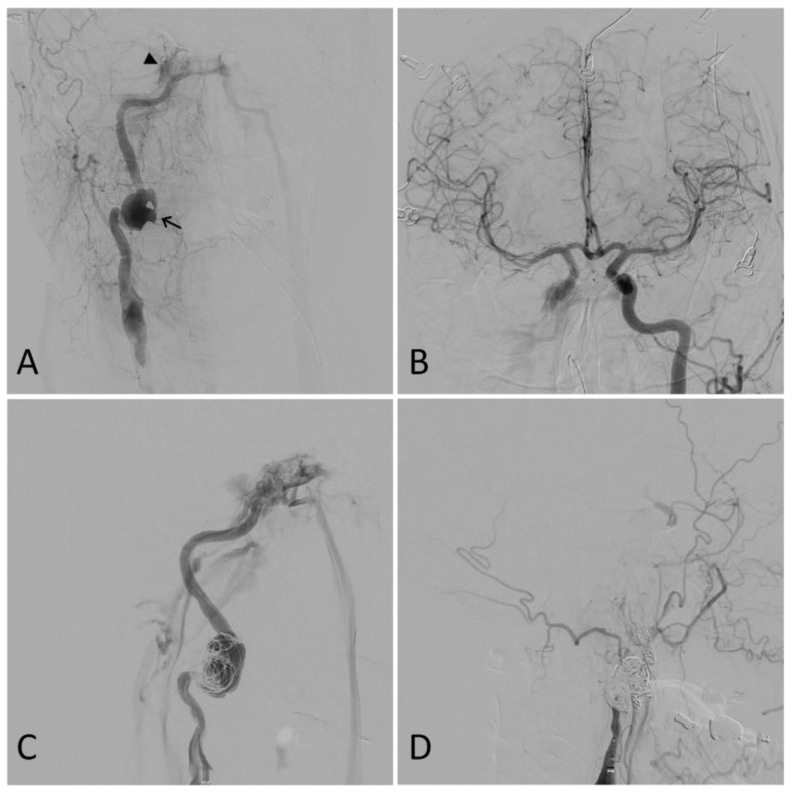
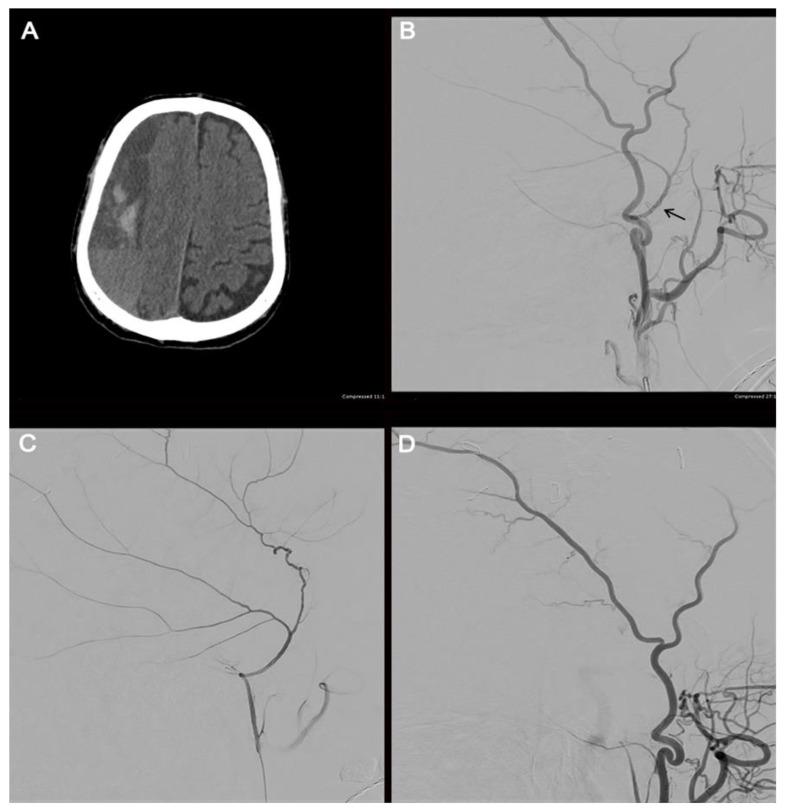
Cerebrovascular injuries resulting from blunt or penetrating trauma to the head and neck often lead to local hemorrhage and stroke. These injuries present with a wide range of manifestations, including carotid or vertebral artery dissection, pseudoaneurysm, occlusion, transection, arteriovenous fistula, carotid-cavernous fistula, epistaxis, venous sinus thrombosis, and subdural hematoma. A selective review of the literature from 1989 to 2023 was conducted to explore various neuroendovascular surgical techniques for craniocervical trauma. A PubMed search was performed using these terms: endovascular, trauma, dissection, blunt cerebrovascular injury, pseudoaneurysm, occlusion, transection, vasospasm, carotid-cavernous fistula, arteriovenous fistula, epistaxis, cerebral venous sinus thrombosis, subdural hematoma, and middle meningeal artery embolization. An increasing array of neuroendovascular procedures are currently available to treat these traumatic injuries. Coils, liquid embolics (onyx or n-butyl cyanoacrylate), and polyvinyl alcohol particles can be used to embolize lesions, while stents, mechanical thrombectomy employing stent-retrievers or aspiration catheters, and balloon occlusion tests and super selective angiography offer additional treatment options based on the specific case. Neuroendovascular techniques prove valuable when surgical options are limited, although comparative data with surgical techniques in trauma cases is limited. Further research is needed to assess the efficacy and outcomes associated with these interventions.
Keywords: angiography; cerebrovascular injuries; craniocervical trauma; head and neck trauma; neuroendovascular surgery; neurointerventional.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Rao P.M., Ivatury R.R., Sharma P., Vinzons A.T., Nassoura Z., Stahl W.M. Cervical vascular injuries: A trauma center experience. Surgery. 1993;114:527–531. - PubMed
-
- Alderazi Y.J., Cruz G.M., Kass-Hout T., Prestigiacomo C.J., Duffis E.J., Gandhi C.D. Endovascular therapy for cerebrovascular injuries after head and neck trauma. Trauma. 2015;17:258–269. doi: 10.1177/1460408615573884. - DOI
Publication types
LinkOut - more resources
Full Text Sources
