

Reduced Lipid Peroxidation Predicts Unfavorable Prognosis in Hepatocellular Carcinoma, but Not Intrahepatic Cholangiocarcinoma
- PMID: 37760911
- PMCID: PMC10525544
- DOI: 10.3390/biomedicines11092471
Reduced Lipid Peroxidation Predicts Unfavorable Prognosis in Hepatocellular Carcinoma, but Not Intrahepatic Cholangiocarcinoma
Abstract
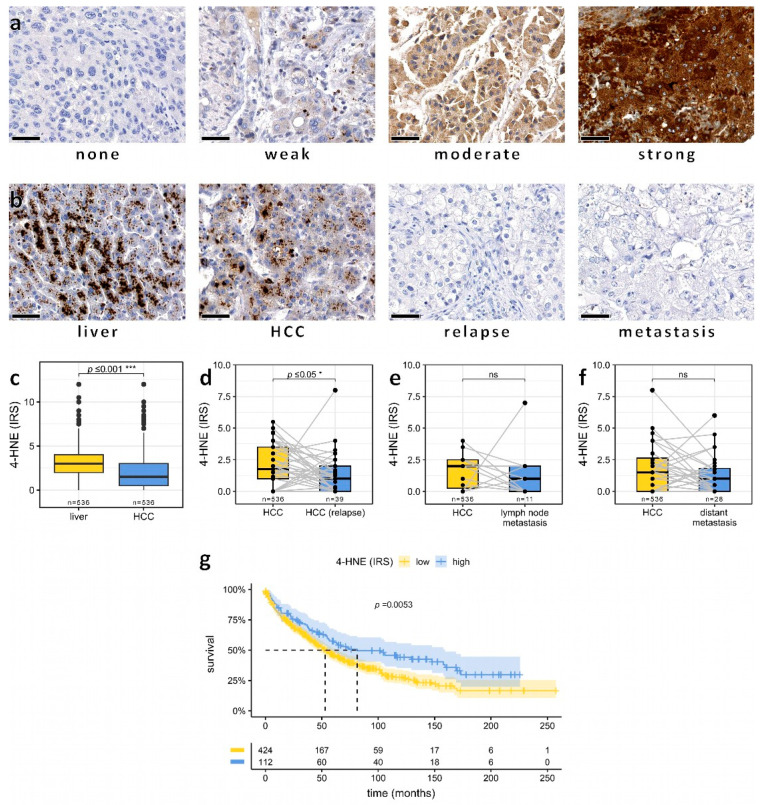
Primary liver cancer, including hepatocellular carcinoma (HCC) and intrahepatic cholangiocarcinoma (iCCA), remains a significant contributor to cancer-related mortality worldwide. Oxidative stress and lipid peroxidation play a key role in chronic liver diseases and have been shown to be pivotal for tumor initiation and progression. 4-hydroxy-nonenal (4-HNE), one of the major mediators of oxidative stress and a well-established biomarker for lipid peroxidation, can act as a signal transducer, inducing inflammation and exerting carcinogenic effects. However, the role of 4-HNE in primary liver cancer remains poorly explored. In this study, we investigated 4-HNE levels in 797 liver carcinomas, including 561 HCC and 236 iCCA, by immunohistochemistry. We then correlated 4-HNE levels with comprehensive clinical data and survival outcomes. In HCC, lower expression levels of 4-HNE were associated with vascular invasion, a high tumor grade, a macrotrabecular-massive HCC subtype, and poor overall survival. Concerning iCCA, large duct iCCA showed significantly higher 4-HNE levels when compared to small duct iCCA. Yet, in iCCA, 4-HNE levels did not correlate with known prognostic parameters or survival outcomes. To conclude, in HCC but not in iCCA, low amounts of 4-HNE predict unfavorable survival outcomes and are associated with aggressive tumor behavior. These findings provide insights into the role of 4-HNE in liver cancer progression and may enable novel therapeutic strategies.
Keywords: 4-HNE; biomarker; hepatocellular carcinoma; intrahepatic cholangiocarcinoma; liver cirrhosis; reactive oxygen species.
Conflict of interest statement
The authors declare no conflict of interest.
Figures




References
-
- Juan C.A., Pérez de la Lastra J.M., Plou F.J., Pérez-Lebeña E. The Chemistry of Reactive Oxygen Species (ROS) Revisited: Outlining Their Role in Biological Macromolecules (DNA, Lipids and Proteins) and Induced Pathologies. Int. J. Mol. Sci. 2021;22:4642. doi: 10.3390/ijms22094642. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
