

Long-Term Clinical Outcome of Abdomino-Thoracic Lymphatic Interventions of Traumatic and Non-Traumatic Lymphatic Leakage in Adults
- PMID: 37760997
- PMCID: PMC10526188
- DOI: 10.3390/biomedicines11092556
Long-Term Clinical Outcome of Abdomino-Thoracic Lymphatic Interventions of Traumatic and Non-Traumatic Lymphatic Leakage in Adults
Abstract
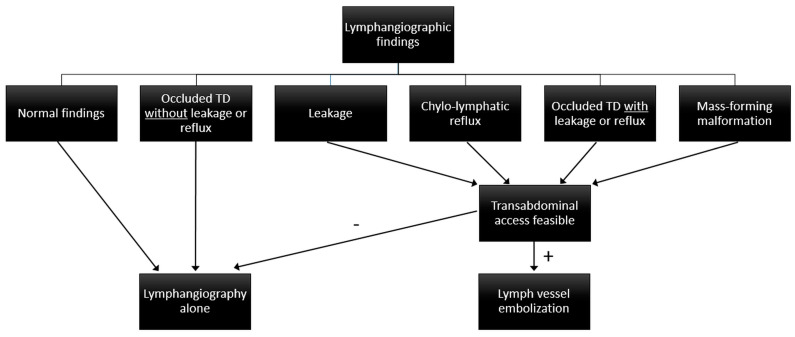
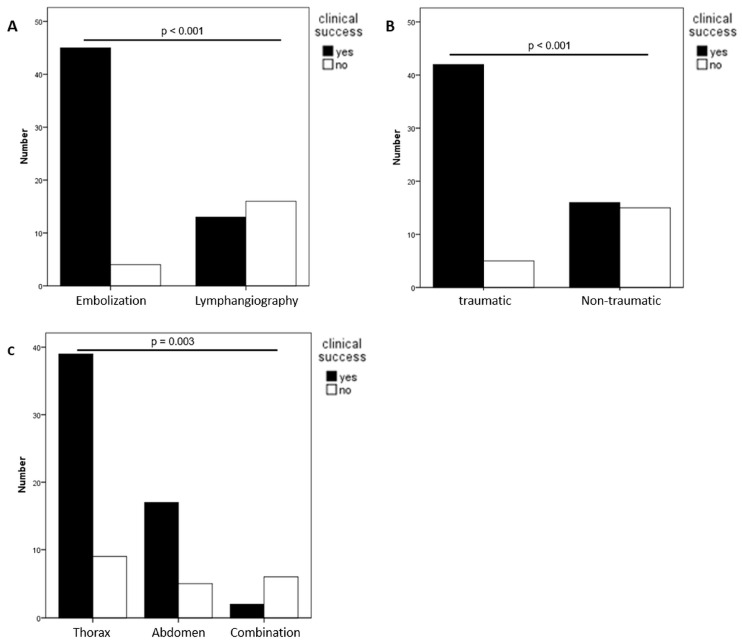
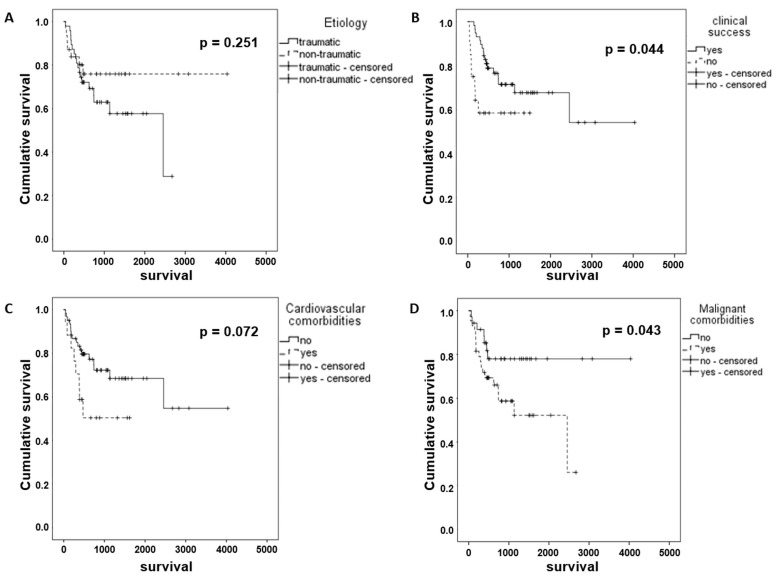
The aim of this study was to retrospectively evaluate the long-term results of lymphatic interventions in adults with abdomino-thoracic lymphatic pathologies. Management of abdomino-thoracic chylous effusions in adults undergoing X-ray-lymphangiography with or without lymph-vessel embolization (LVE) from 2010-2018 was reviewed. Patients underwent lymphangiography alone when imaging showed normal findings or lymphatic obstruction without leakage or reflux; otherwise, LVE was performed (leakage, reflux, obstruction with leakage or reflux, lymphatic masses). Technical and clinical success, complications, and long-term outcomes were assessed. 78 patients (47 male, median age 56.3 years) were treated for chylous effusions (60.3% traumatic, 39.7% non-traumatic). Lymphangiography showed leakage (48.7%), reflux (14.1%), obstruction (28.2%), lymphatic masses (5.1%), and normal findings (3.8%). Embolization was performed in 49/78 (62.8%) cases. Overall, treatment was clinically successful in 74.4% (mean follow-up of 28 months), with significant differences between LVE and lymphangiography (91.8% vs. 44.8%; p < 0.001), traumatic and non-traumatic etiologies (89.4% vs. 51.6%; p < 0.001), and leakage locations (p = 0.003). The clinical success of LVE did not differ between leakage etiologies or locations. Complications occurred in 5 patients (2/5 needed treatment). Patients survived significantly longer after successful treatment (2679 vs. 927 days; p = 0.044) and without malignancy (3214 vs. 1550 days; p = 0.043). Lymphatic interventions are safe and effective. LVE should be attempted whenever feasible, as success is high (>90%). Successful intervention has a positive effect on patient survival.
Keywords: chylothorax; chylous ascites; lymphangiography.
Conflict of interest statement
There are no financial arrangements that could be regarded as a conflict of interest in connection with the present work. Financial connections outside the present work: JAL: Speakers Bureau: Philips Healthcare (Netherlands), Bayer Vital (Germany); UIA: Speakers Bureau: Siemens Healthineers (Erlangen, Germany), CCP: Speakers Bureau: Philips Healthcare (Best, Netherlands), Bayer Vital (Germany), Guerbet (France), Julius Zorn GmbH (Germany).
Figures
References
-
- Pieper C.C., Hur S., Sommer C.M., Nadolski G., Maleux G., Kim J., Itkin M. Back to the Future: Lipiodol in Lymphography-From Diagnostics to Theranostics. Investig. Radiol. 2019;54:600–615. - PubMed
-
- Nadolski G. Nontraumatic Chylothorax: Diagnostic Algorithm and Treatment Options. Tech. Vasc. Interv. Radiol. 2016;19:286–290. - PubMed
LinkOut - more resources
Full Text Sources
