

Similarities and Differences between Multisystem Inflammatory Syndrome in Children (MIS-C) and Kawasaki Disease Shock Syndrome
- PMID: 37761488
- PMCID: PMC10527784
- DOI: 10.3390/children10091527
Similarities and Differences between Multisystem Inflammatory Syndrome in Children (MIS-C) and Kawasaki Disease Shock Syndrome
Abstract
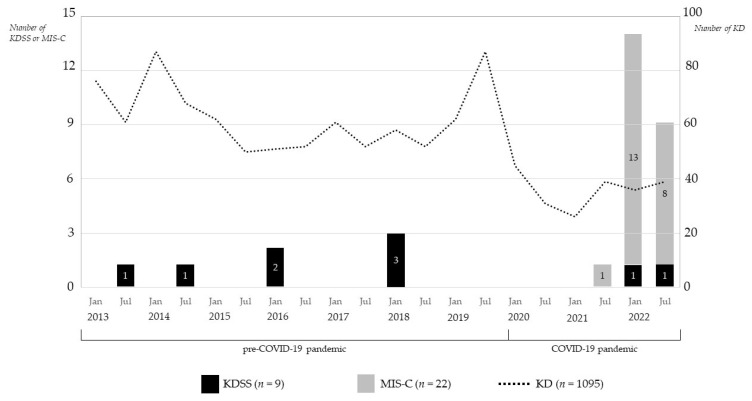
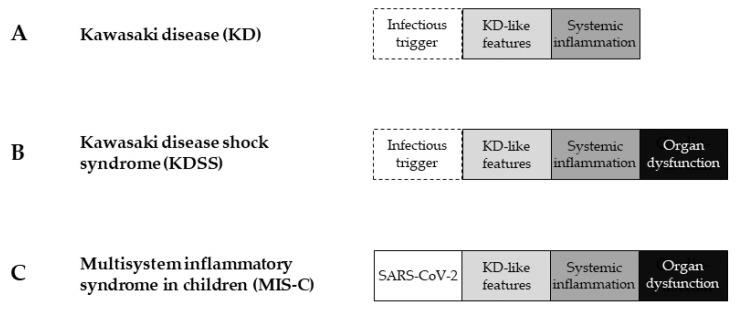
This study aimed to investigate the characteristics of COVID-19-associated multisystem inflammatory syndrome in children (MIS-C) and Kawasaki disease shock syndrome (KDSS) and to compare the similarities and differences between the two diseases. The incidence of KDSS and MIS-C was also estimated. Medical records of patients diagnosed with MIS-C or KDSS at four hospitals from January 2013 to December 2022 were retrospectively reviewed. Thirty-one patients were enrolled in the study in either an MIS-C group (n = 22) or a KDSS group (n = 9). The incidence of KDSS in KD was 0.8% (9/1095) and the incidence of MIS-C versus KD was 10.2% (22/216). Compared with the MIS-C group, the KDSS group had longer hospital stays and more severe systemic inflammation (e.g., anemia, elevated C-reactive protein, hypoalbuminemia, and pyuria) and organ dysfunction (e.g., number of involved organs, shock, vasoactive infusion, and intensive care unit admission). All patients in the MIS-C group, but none in the KDSS group, including two patients during the COVID-19 pandemic, had laboratory evidence of SARS-CoV-2 infection. MIS-C and KDSS shared demographic, clinical, and laboratory characteristics; organ dysfunction; treatment; and outcomes. Overall severity was more severe in patients with KDSS than in those with MIS-C. The most important difference between MIS-C and KDSS was whether SARS-CoV-2 was identified as an infectious trigger.
Keywords: Kawasaki disease; Kawasaki disease shock syndrome; multisystem inflammatory syndrome in children.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Schlapbach L.J., Andre M.C., Grazioli S., Schöbi N., Ritz N., Aebi C., Agyeman P., Albisetti M., Bailey D.G.N., Berger C., et al. Best Practice Recommendations for the diagnosis and management of children with pediatric inflammatory multisystem syndrome temporally associated with SARS-CoV-2 (PIMS-TS; multisystem inflammatory syndrome in children, MIS-C) in Switzerland. Front. Pediatr. 2021;9:667507. doi: 10.3389/fped.2021.667507. - DOI - PMC - PubMed
-
- Verdoni L., Mazza A., Gervasoni A., Martelli L., Ruggeri M., Ciuffreda M., Bonanomi E., D’Antiga L. An outbreak of severe Kawasaki-like disease at the Italian epicentre of the SARS-CoV-2 Epidemic: An observational cohort study. Lancet. 2020;395:1771–1778. doi: 10.1016/S0140-6736(20)31103-X. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
