

Oral Iron Absorption of Ferric Citrate Hydrate and Hepcidin-25 in Hemodialysis Patients: A Prospective, Multicenter, Observational Riona-Oral Iron Absorption Trial
- PMID: 37762085
- PMCID: PMC10531220
- DOI: 10.3390/ijms241813779
Oral Iron Absorption of Ferric Citrate Hydrate and Hepcidin-25 in Hemodialysis Patients: A Prospective, Multicenter, Observational Riona-Oral Iron Absorption Trial
Abstract
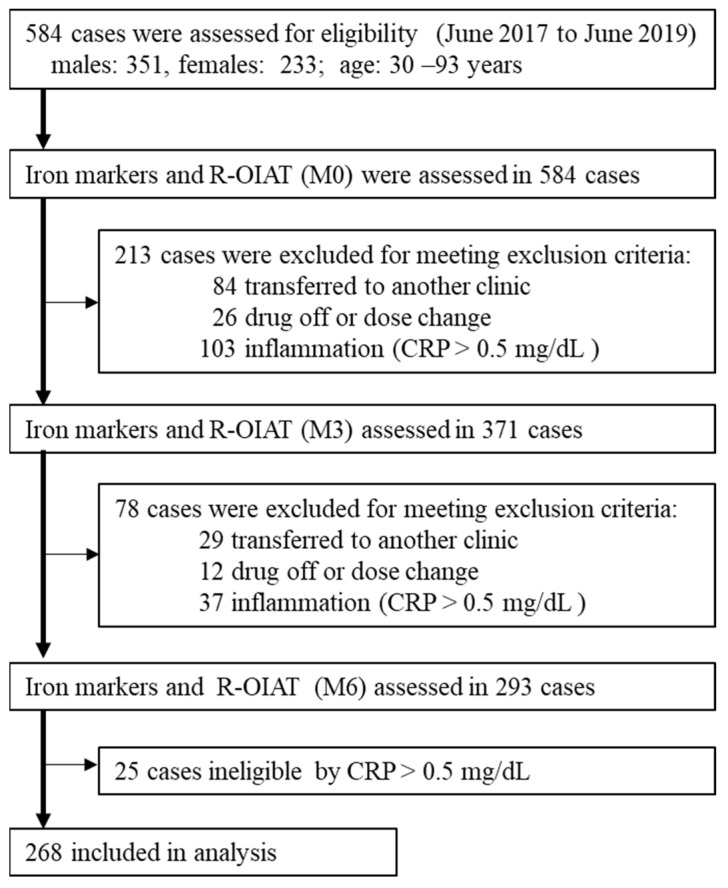
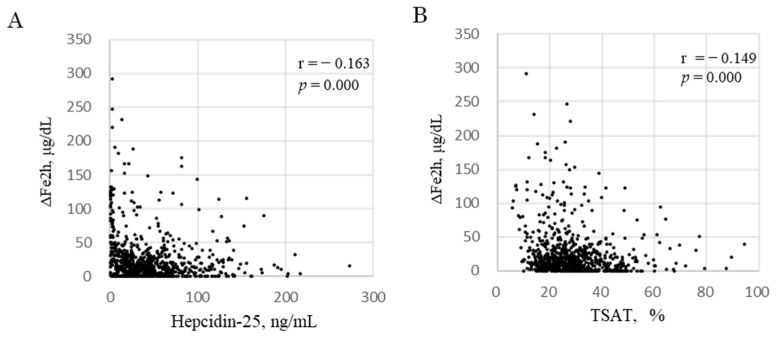
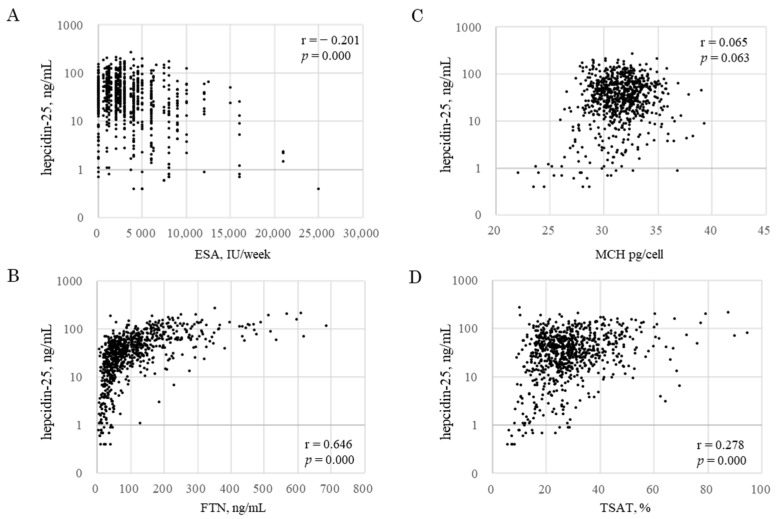
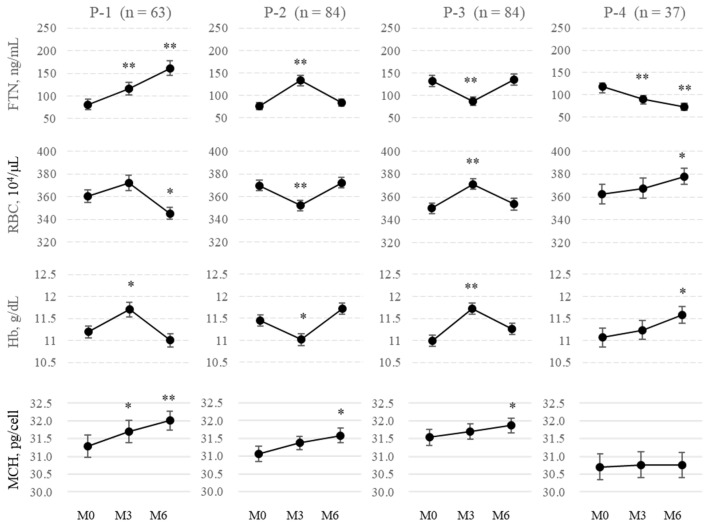
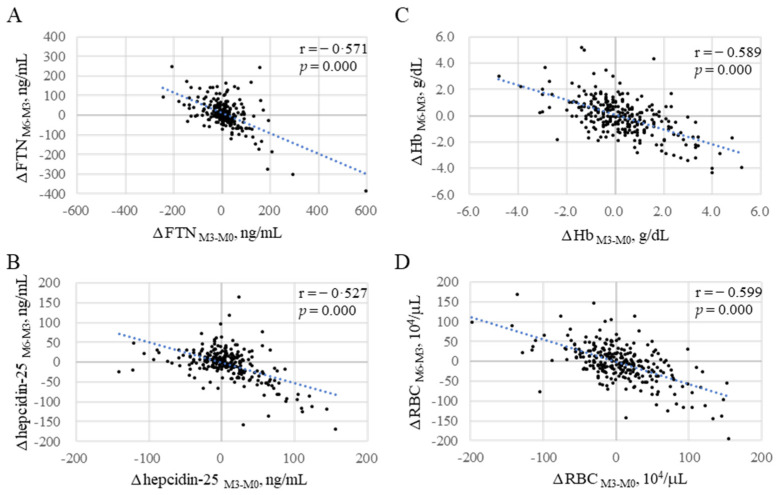
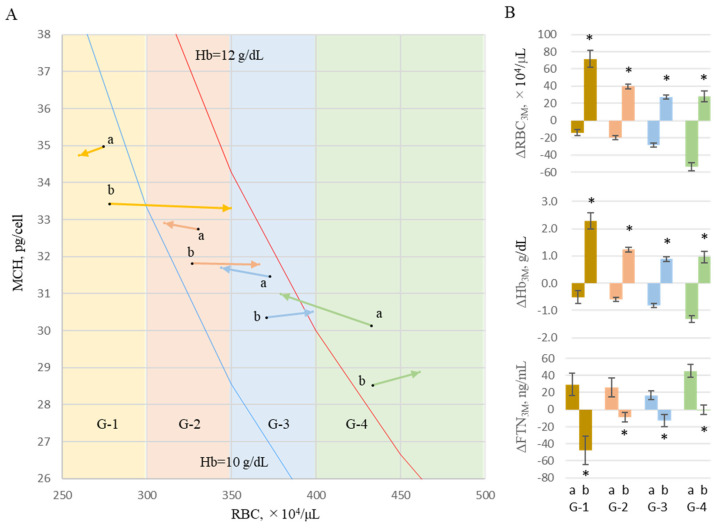
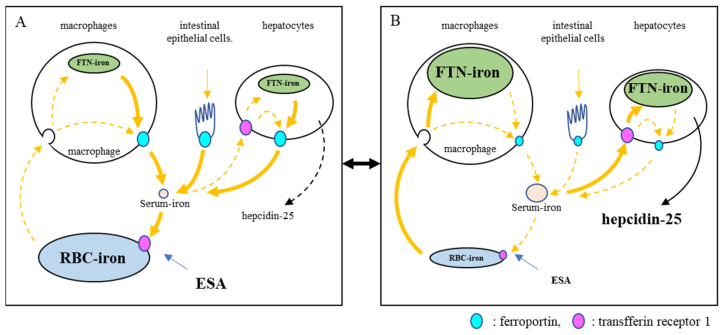
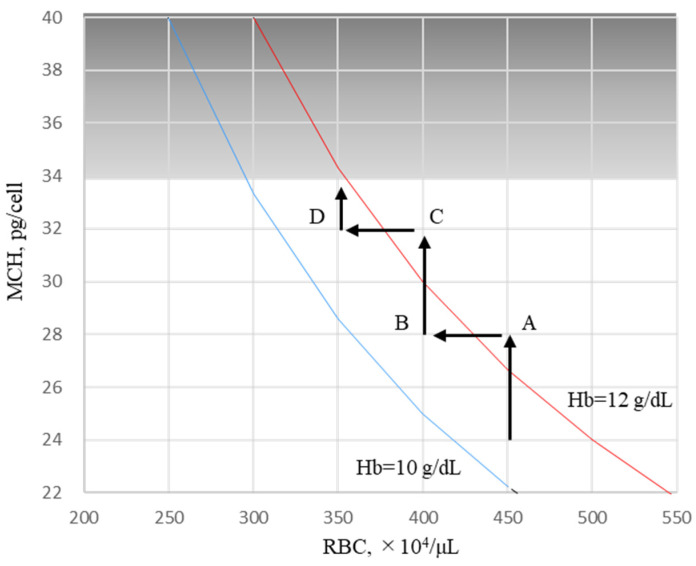
Oral ferric citrate hydrate (FCH) is effective for iron deficiencies in hemodialysis patients; however, how iron balance in the body affects iron absorption in the intestinal tract remains unclear. This prospective observational study (Riona-Oral Iron Absorption Trial, R-OIAT, UMIN 000031406) was conducted at 42 hemodialysis centers in Japan, wherein 268 hemodialysis patients without inflammation were enrolled and treated with a fixed amount of FCH for 6 months. We assessed the predictive value of hepcidin-25 for iron absorption and iron shift between ferritin (FTN) and red blood cells (RBCs) following FCH therapy. Serum iron changes at 2 h (ΔFe2h) after FCH ingestion were evaluated as iron absorption. The primary outcome was the quantitative delineation of iron variables with respect to ΔFe2h, and the secondary outcome was the description of the predictors of the body's iron balance. Generalized estimating equations (GEEs) were used to identify the determinants of iron absorption during each phase of FCH treatment. ΔFe2h increased when hepcidin-25 and TSAT decreased (-0.459, -0.643 to -0.276, p = 0.000; -0.648, -1.099 to -0.197, p = 0.005, respectively) in GEEs. FTN increased when RBCs decreased (-1.392, -1.749 to -1.035, p = 0.000) and hepcidin-25 increased (0.297, 0.239 to 0.355, p = 0.000). Limiting erythropoiesis to maintain hemoglobin levels induces RBC reduction in hemodialysis patients, resulting in increased hepcidin-25 and FTN levels. Hepcidin-25 production may prompt an iron shift from RBC iron to FTN iron, inhibiting iron absorption even with continued FCH intake.
Keywords: ferric citrate hydrate; hemodialysis; hepcidin-25; iron shift; oral iron absorption.
Conflict of interest statement
Tomosugi is a professor at Kanazawa Medical University and the president of Medical Care Proteomics Biotechnology Co., Ltd. However, this association did not alter the authors’ adherence to all policies regarding the sharing of data. The authors have declared that no conflict of interest exist.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
