

Postprandial Hyperlipidemia: Its Pathophysiology, Diagnosis, Atherogenesis, and Treatments
- PMID: 37762244
- PMCID: PMC10530470
- DOI: 10.3390/ijms241813942
Postprandial Hyperlipidemia: Its Pathophysiology, Diagnosis, Atherogenesis, and Treatments
Abstract
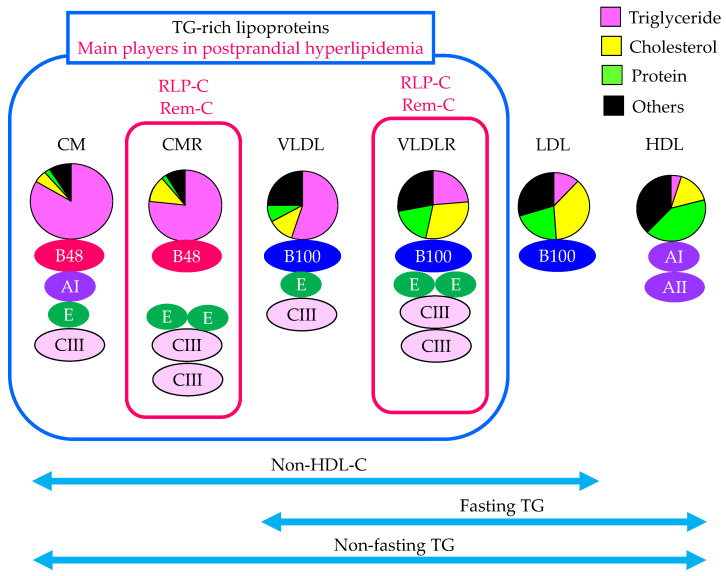
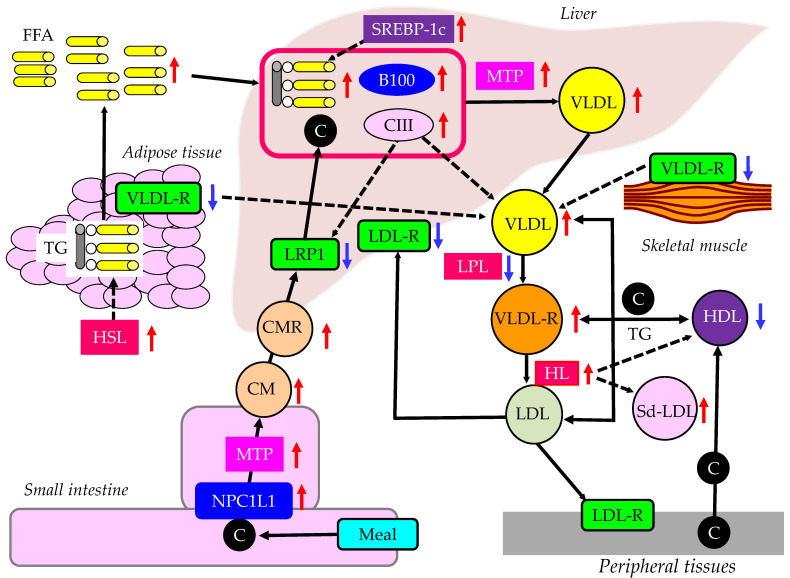
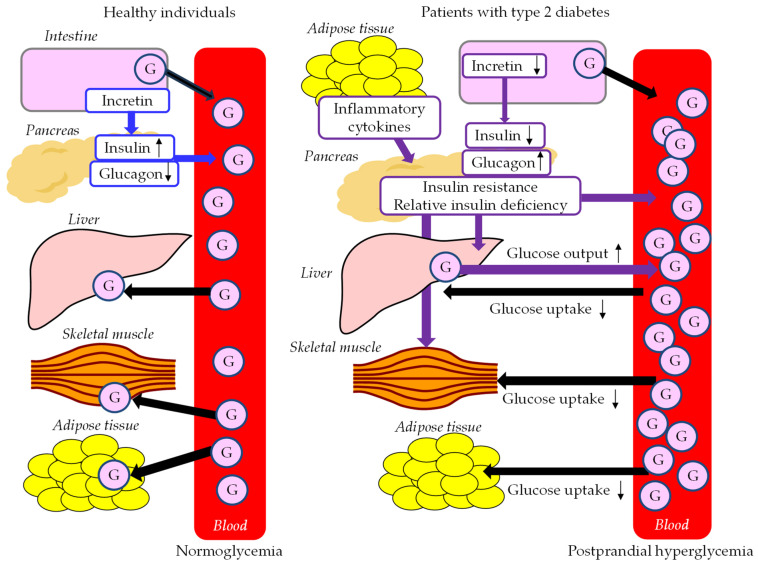
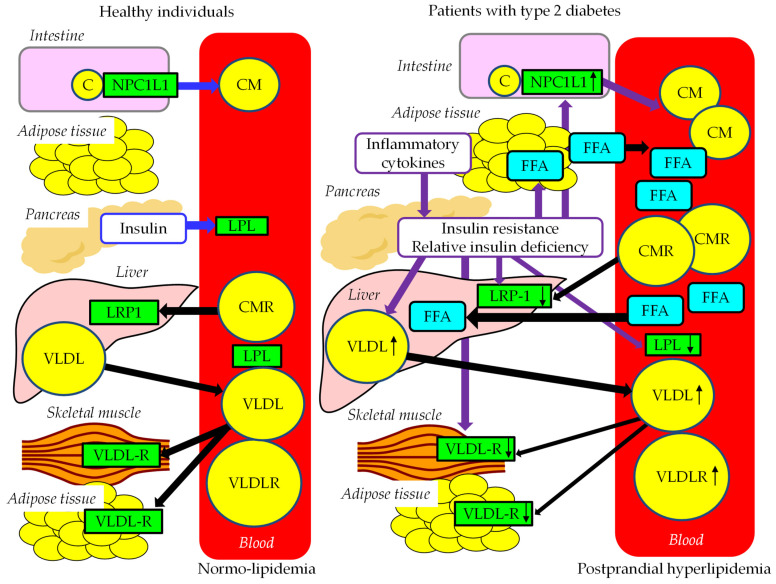
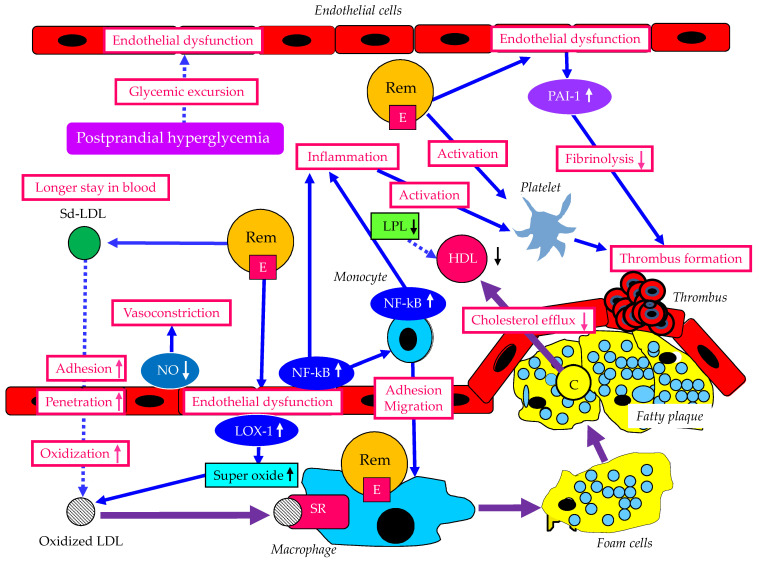
Postprandial hyperlipidemia showing postprandial increases in serum triglyceride (TG) is associated with the development of atherosclerotic cardiovascular disease (ASCVD). To diagnose postprandial hyperlipidemia, the oral fat loading test (OFLT) should be performed; however, this test is very time-consuming and is difficult to perform. Elevated serum TG levels reflect an increase in TG-rich lipoproteins (TRLs), such as chylomicrons (CM), very low-density lipoproteins (VLDL), and their remnants (CM remnants [CMRs] and VLDL remnants [VLDLRs]). Understanding of elevation in CMR and/or VLDLR can lead us to understand the existence of postprandial hyperlipidemia. The measurement of apo B48, which is a constituent of CM and CMR; non-fasting TG, which includes TG content in all lipoproteins including CM and CMR; non-high-density lipoprotein cholesterol (non-HDL-C), which includes TRLs and low-density lipoprotein; and remnant cholesterol are useful to reveal the existence of postprandial hyperlipidemia. Postprandial hyperlipidemia is observed in patients with familial type III hyperlipoproteinemia, familial combined hyperlipidemia, chronic kidney disease, metabolic syndrome and type 2 diabetes. Postprandial hyperlipidemia is closely related to postprandial hyperglycemia, and insulin resistance may be an inducing and enhancing factor for both postprandial hyperlipidemia and postprandial hyperglycemia. Remnant lipoproteins and metabolic disorders associated with postprandial hyperlipidemia have various atherogenic properties such as induction of inflammation and endothelial dysfunction. A healthy diet, calorie restriction, weight loss, and exercise positively impact postprandial hyperlipidemia. Anti-hyperlipidemic drugs such pemafibrate, fenofibrate, bezafibrate, ezetimibe, and eicosapentaenoic acid have been shown to improve postprandial hyperlipidemia. Anti-diabetic drugs including metformin, alpha-glucosidase inhibitors, pioglitazone, dipeptidyl-peptidase-4 inhibitors and glucagon-like peptide 1 analogues have been shown to ameliorate postprandial hyperlipidemia. Although sodium glucose cotransporter-2 inhibitors have not been proven to reduce postprandial hyperlipidemia, they reduced fasting apo B48 and remnant lipoprotein cholesterol. In conclusion, it is important to appropriately understand the existence of postprandial hyperlipidemia and to connect it to optimal treatments. However, there are some problems with the diagnosis for postprandial hyperlipidemia. Postprandial hyperlipidemia cannot be specifically defined by measures such as TG levels 2 h after a meal. To study interventions for postprandial hyperlipidemia with the outcome of preventing the onset of ASCVD, it is necessary to define postprandial hyperlipidemia using reference values such as IGT.
Keywords: apo B48; cardiovascular disease; insulin resistance; postprandial hyperlipidemia; remnant cholesterol; small dense LDL.
Conflict of interest statement
The authors declare no conflict of interest in relation to the present review paper.
Figures
Similar articles
-
Postprandial remnant-like lipoproteins in hypertriglyceridemia.J Clin Endocrinol Metab. 2001 Jul;86(7):3134-42. doi: 10.1210/jcem.86.7.7627. J Clin Endocrinol Metab. 2001. PMID: 11443178
-
Postprandial Hyperlipidemia and Remnant Lipoproteins.J Atheroscler Thromb. 2017 Feb 1;24(2):95-109. doi: 10.5551/jat.RV16003. Epub 2016 Nov 8. J Atheroscler Thromb. 2017. PMID: 27829582 Free PMC article. Review.
-
Postprandial hyperlipidemia as a potential residual risk factor.J Cardiol. 2016 Apr;67(4):335-9. doi: 10.1016/j.jjcc.2015.12.001. Epub 2015 Dec 29. J Cardiol. 2016. PMID: 26744235 Review.
-
Fasting remnant lipoproteins can predict postprandial hyperlipidemia.Lipids Health Dis. 2012 Oct 31;11:146. doi: 10.1186/1476-511X-11-146. Lipids Health Dis. 2012. PMID: 23110373 Free PMC article.
-
Preferential reduction of very low density lipoprotein-1 particle number by fenofibrate in type IIB hyperlipidemia: consequences for lipid accumulation in human monocyte-derived macrophages.Atherosclerosis. 2001 Mar;155(1):251-60. doi: 10.1016/s0021-9150(00)00634-1. Atherosclerosis. 2001. PMID: 11223449 Clinical Trial.
Cited by
-
The chylomicron saga: time to focus on postprandial metabolism.Front Endocrinol (Lausanne). 2024 Jan 18;14:1322869. doi: 10.3389/fendo.2023.1322869. eCollection 2023. Front Endocrinol (Lausanne). 2024. PMID: 38303975 Free PMC article. Review.
-
Bile acids and incretins as modulators of obesity-associated atherosclerosis.Front Cardiovasc Med. 2025 Jan 6;11:1510148. doi: 10.3389/fcvm.2024.1510148. eCollection 2024. Front Cardiovasc Med. 2025. PMID: 39834741 Free PMC article. Review.
-
Role of intestinal testosterone-degrading bacteria and 3/17β-HSD in the pathogenesis of testosterone deficiency-induced hyperlipidemia in males.NPJ Biofilms Microbiomes. 2024 Nov 9;10(1):123. doi: 10.1038/s41522-024-00599-1. NPJ Biofilms Microbiomes. 2024. PMID: 39521773 Free PMC article.
-
Advances in Gut Microbiota-Targeted Therapeutics for Metabolic Syndrome.Microorganisms. 2024 Apr 24;12(5):851. doi: 10.3390/microorganisms12050851. Microorganisms. 2024. PMID: 38792681 Free PMC article. Review.
-
Metabolic Dysfunction-Associated Steatotic Liver Disease: Pathogenetic Links to Cardiovascular Risk.Biomolecules. 2025 Jan 22;15(2):163. doi: 10.3390/biom15020163. Biomolecules. 2025. PMID: 40001466 Free PMC article. Review.
References
-
- Nikkilä M., Solakivi T., Lehtimäki T., Koivula T., Laippala P., Aström B. Postprandial plasma lipoprotein changes in relation to apolipoprotein E phenotypes and low density lipoprotein size in men with and without coronary artery disease. Atherosclerosis. 1994;106:149–157. doi: 10.1016/0021-9150(94)90120-1. - DOI - PubMed
-
- Chen Y.D., Skowronski R., Coulston A.M., Pietarinen J., Hollenbeck C.B., Reaven G.M. Effect of acute variations in dietary fat and carbohydrate intake on retinyl ester content of intestinally derived lipoproteins. J. Clin. Endocrinol. Metab. 1992;74:28–32. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
