

The Heart and Seizures: Friends or Enemies?
- PMID: 37762746
- PMCID: PMC10532013
- DOI: 10.3390/jcm12185805
The Heart and Seizures: Friends or Enemies?
Abstract
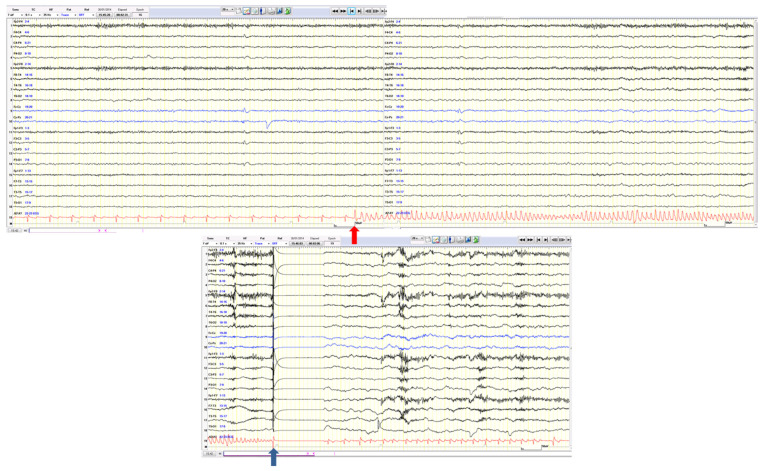
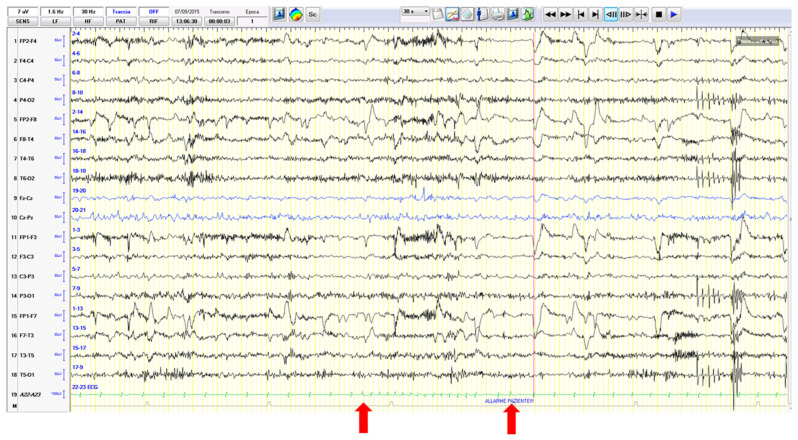
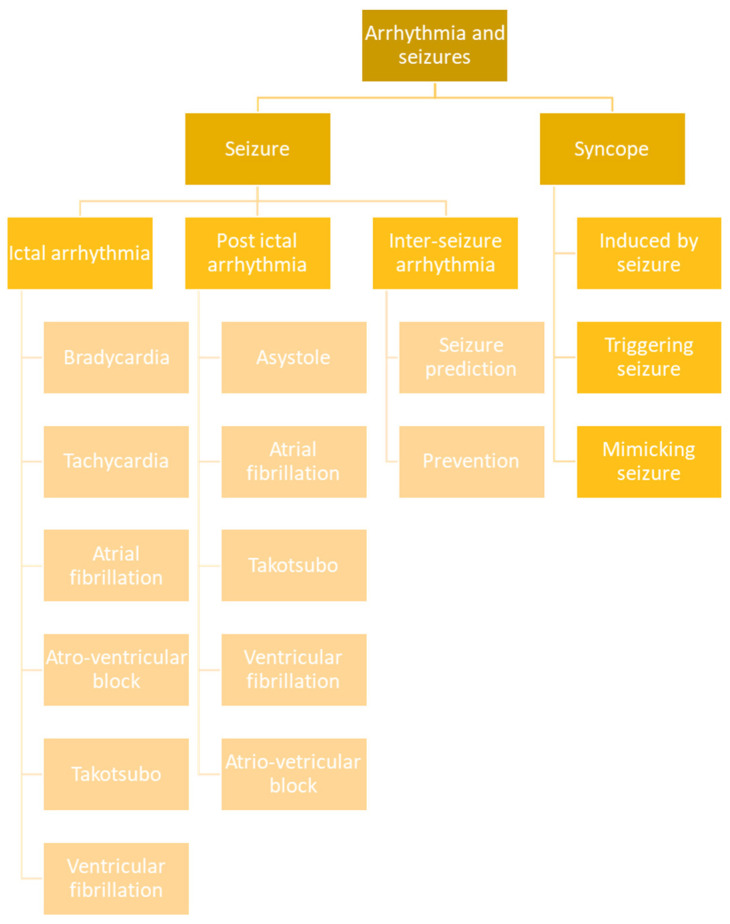
The heart and seizures are closely linked by an indissoluble relationship that finds its basis in the cerebral limbic circuit whose mechanisms remain largely obscure. The differential diagnosis between seizures and syncopes has always been a cornerstone of the collaboration between cardiologists and neurologists and is renewed as a field of great interest for multidisciplinary collaboration in the era of the diffusion of prolonged telemonitoring units. The occurrence of ictal or post-ictal arrhythmias is currently a cause of great scientific debate with respect to the role and risks that these complications can generate (including sudden unexpected death in epilepsy). Furthermore, the study of epileptic seizures and the arrhythmological complications they cause (during and after seizures) also allows us to unravel the mechanisms that link them. Finally, intercritical arrhythmias may represent great potential in terms of the prevention of cardiological risk in epileptic patients as well as in the possible prediction of the seizures themselves. In this paper, we review the pertaining literature on this subject and propose a scheme of classification of the cases of arrhythmia temporally connected to seizures.
Keywords: SUDEP; arrhythmia; epilepsy; ictal asystole; loss of consciousness; syncope.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
