

Functional (Re)Development of SYNTAX Score II 2020: Predictive Performance and Risk Assessment
- PMID: 37762785
- PMCID: PMC10531756
- DOI: 10.3390/jcm12185844
Functional (Re)Development of SYNTAX Score II 2020: Predictive Performance and Risk Assessment
Abstract
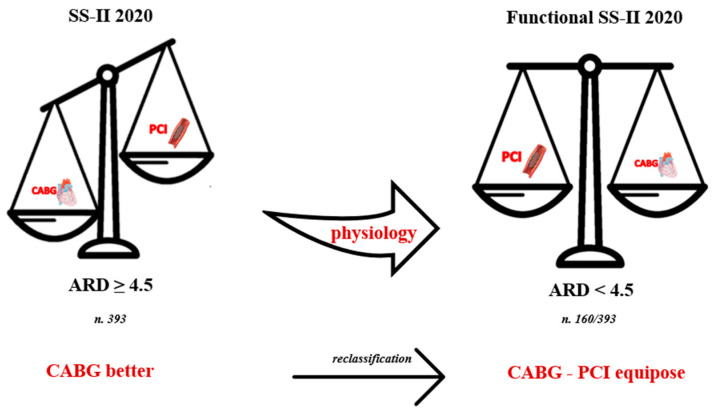
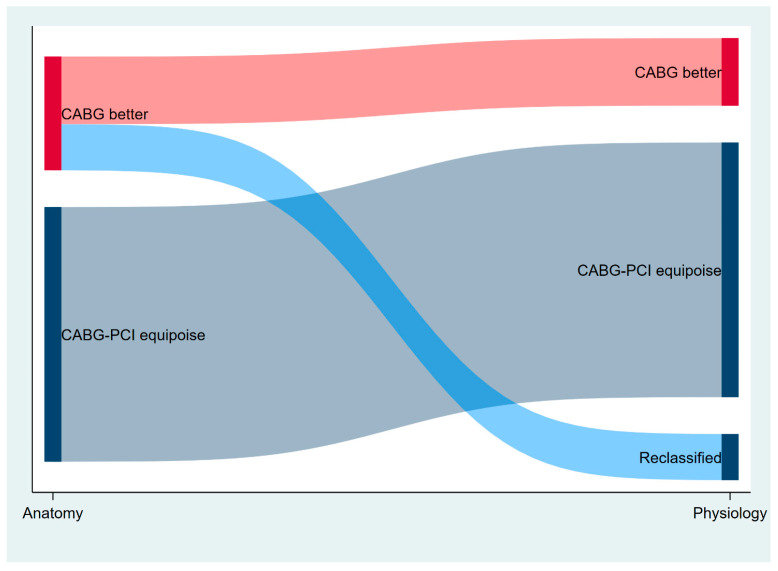
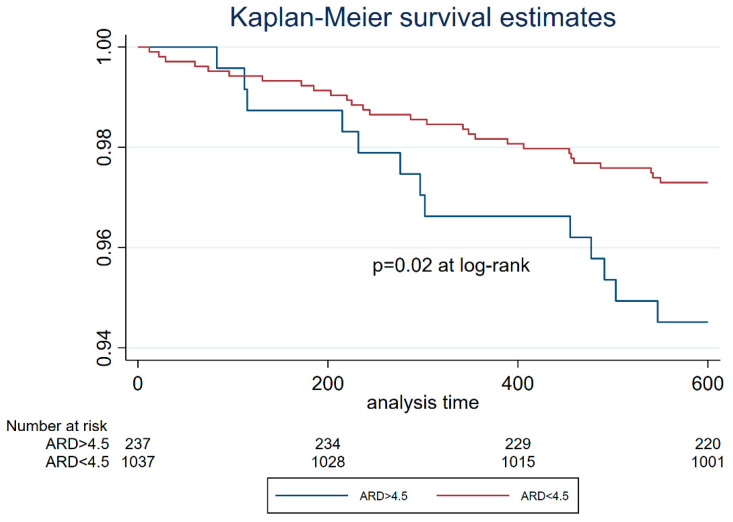
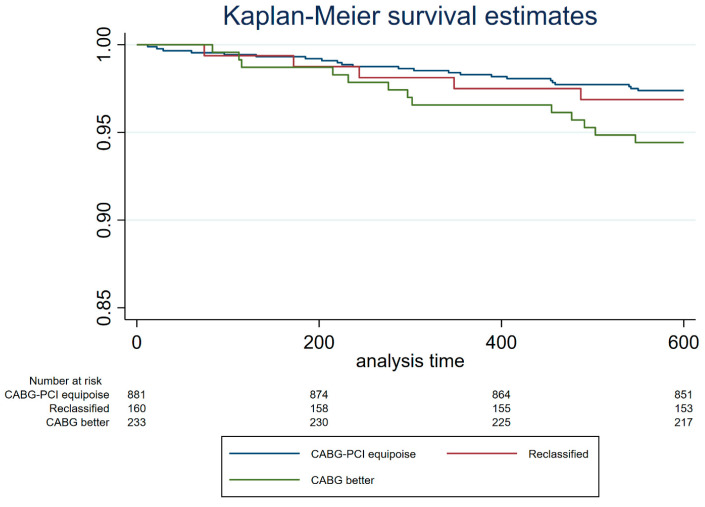
The present study investigates the prognostic value of the Syntax Score II 2020 corrected for flow-limiting lesions and its ability to better address treatment by benefit prediction among patients with left main or multivessel disease. We analyzed 1274 patients from the HALE-BOPP cohort and integrated the Syntax Score II 2020 with the result of the fractional flow reserve (FFR) evaluation. Absolute risk difference (ARD) between surgical and percutaneous revascularization was calculated for anatomic and functional Syntax Score II 2020 predicted mortality. The ARD allowed to stratify the population into two large categories: "coronary artery bypass graft (CABG) better" with ARD ≥ 4.5% and "CABG-percutaneous coronary intervention (PCI) equipoise" with ARD < 4.5%. The mean global anatomical Syntax Score was 15.5 ± 9.2, whereas the functional one was 9.5 ± 10 (p < 0.01). Using the anatomic Syntax Score II 2020, 881 patients had a CABG-PCI equipoise. This number increased to 1041 after considering only flow-limiting lesions by FFR (p < 0.001); therefore, 40% of CABG better patients were reclassified within the CABG-PCI equipoise category. Kaplan-Maier curves showed similar actual survival rates for patients originally with CABG-PCI equipoise and those reclassified, in both cases higher than those from CABG better patients (p < 0.01). The integration between Syntax Score II 2020 and physiology is feasible, and merging clinical, anatomic and functional data allows for better risk prediction and therapeutic guidance.
Keywords: fractional flow reserve; multivessel disease; syntax score.
Conflict of interest statement
The authors declare no conflict of interest. The funders had no role in the design of the study, in the collection, analyses, or interpretation of data, in the writing of the manuscript, or in the decision to publish the results.
Figures
References
-
- Hlatky M.A., Boothroyd D.B., Bravata D.M., Boersma E., Booth J., Brooks M.M., Carrié D., Clayton T.C., Danchin N., Flather M., et al. Coronary Artery Bypass Surgery Compared with Percutaneous Coronary Interventions for Multivessel Disease: A Collaborative Analysis of Individual Patient Data from Ten Randomised Trials. Lancet. 2009;373:1190–1197. doi: 10.1016/S0140-6736(09)60552-3. - DOI - PubMed
-
- Fearon W.F., Zimmermann F.M., de Bruyne B., Piroth Z., van Straten A.H.M., Szekely L., Davidavičius G., Kalinauskas G., Mansour S., Kharbanda R., et al. Fractional Flow Reserve–Guided PCI as Compared with Coronary Bypass Surgery. N. Engl. J. Med. 2022;386:128–137. doi: 10.1056/NEJMoa2112299. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
