

Assessing Continuous Epidural Infusion and Programmed Intermittent Epidural Bolus for Their Effectiveness in Providing Labor Analgesia: A Mono-Centric Retrospective Comparative Study
- PMID: 37763698
- PMCID: PMC10535284
- DOI: 10.3390/medicina59091579
Assessing Continuous Epidural Infusion and Programmed Intermittent Epidural Bolus for Their Effectiveness in Providing Labor Analgesia: A Mono-Centric Retrospective Comparative Study
Abstract
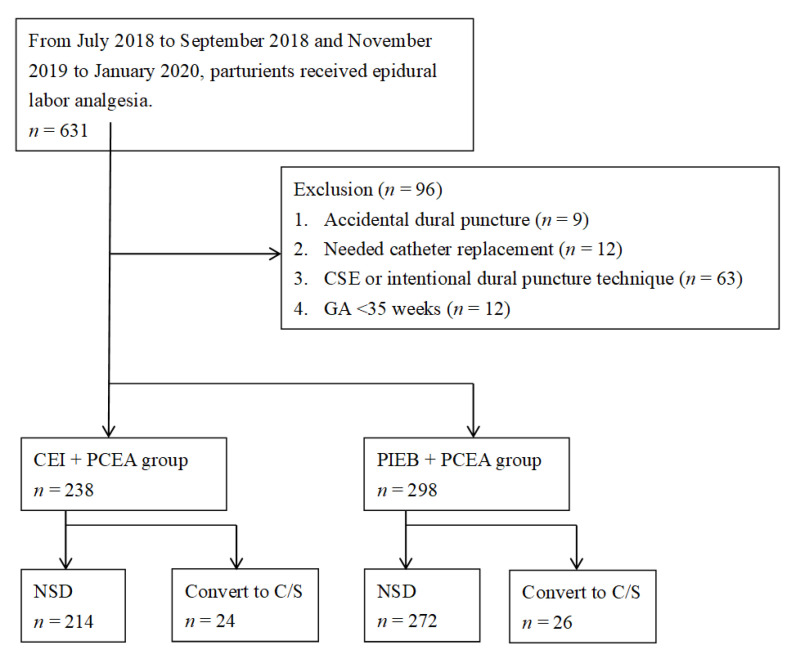
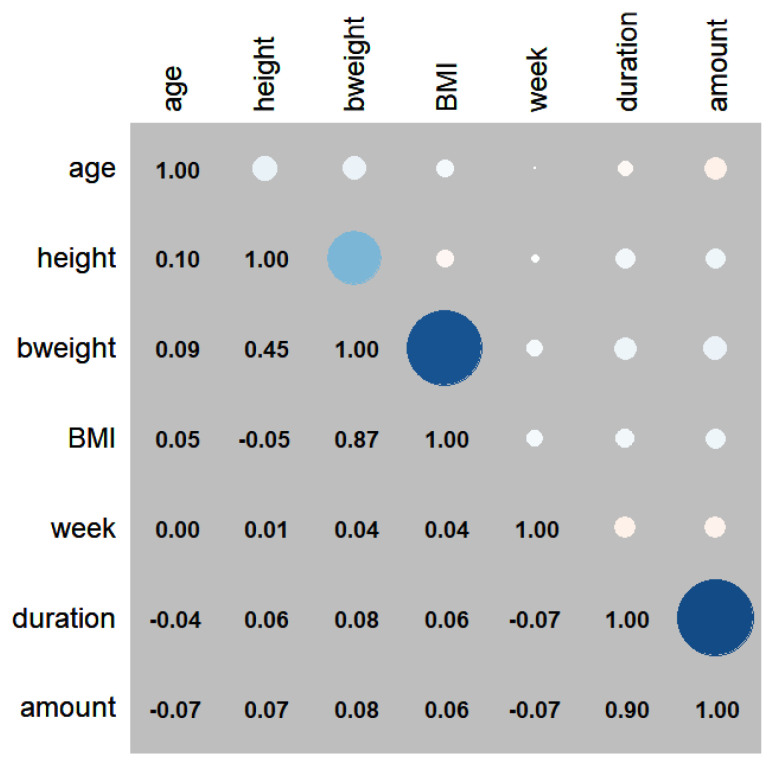
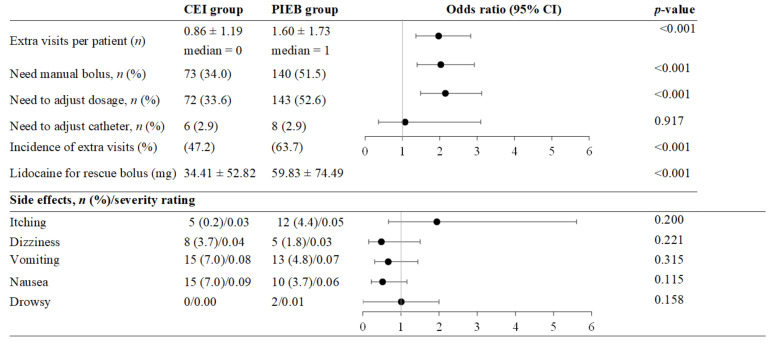
Background and Objectives: Local anesthetics administered via epidural catheters have evolved from intermittent top-ups to simultaneous administration of continuous epidural infusion (CEI) and patient-controlled epidural analgesia (PCEA) using the same device. The latest programmed intermittent epidural bolus (PIEB) model is believed to create a wider and more even distribution of analgesia inside the epidural space. The switch from CEI + PCEA to PIEB + PCEA in our department began in 2018; however, we received conflicting feedback regarding workload from the quality assurance team. This study aimed to investigate the benefits and drawbacks of this conversion, including the differences in acute pain service (APS) staff workload, maternal satisfaction, side effects, and complications before and after the changeover. Materials and Methods: Items from the APS records included total delivery time, average local anesthetic dosage, and the formerly mentioned items. The incidence of side effects, the association between the duration of delivery and total dosage, and hourly medication usage in the time subgroups of the CEI and PIEB groups were compared. The staff workload incurred from rescue bolus injection, catheter adjustment, and dosage adjustment was also analyzed. Results: The final analysis included 214 and 272 cases of CEI + PCEA and PIEB + PCEA for labor analgesia, respectively. The total amount of medication and average hourly dosage were significantly lower in the PIEB + PCEA group. The incidences of dosage change, manual bolus, extra visits per patient, and lidocaine use for rescue bolus were greater in the PIEB + PCEA group, indicating an increased staff workload. However, the two groups did not differ in CS rates, labor time, maternal satisfaction, and side effects. Conclusions: This study revealed that while PIEB + PCEA maintained the advantage of decreasing total drug doses, it inadvertently increased the staff burden. Increased workload might be a consideration in clinical settings when choosing between different methods of PCEA.
Keywords: analgesia; anesthesia; epidural; labor pain; patient-controlled; workload.
Conflict of interest statement
The authors declare no conflict of interest.
Figures


References
-
- Smith A., Laflamme E., Komanecky C. Pain management in labor. Am. Fam. Physician. 2021;103:355–364. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
