

Endovascular Treatment of Visceral Artery Pseudoaneurysms with Ethylene-Vinyl Alcohol (EVOH) Copolymer-Based Non-Adhesive Liquid Embolic Agents (NALEAs)
- PMID: 37763725
- PMCID: PMC10537405
- DOI: 10.3390/medicina59091606
Endovascular Treatment of Visceral Artery Pseudoaneurysms with Ethylene-Vinyl Alcohol (EVOH) Copolymer-Based Non-Adhesive Liquid Embolic Agents (NALEAs)
Abstract
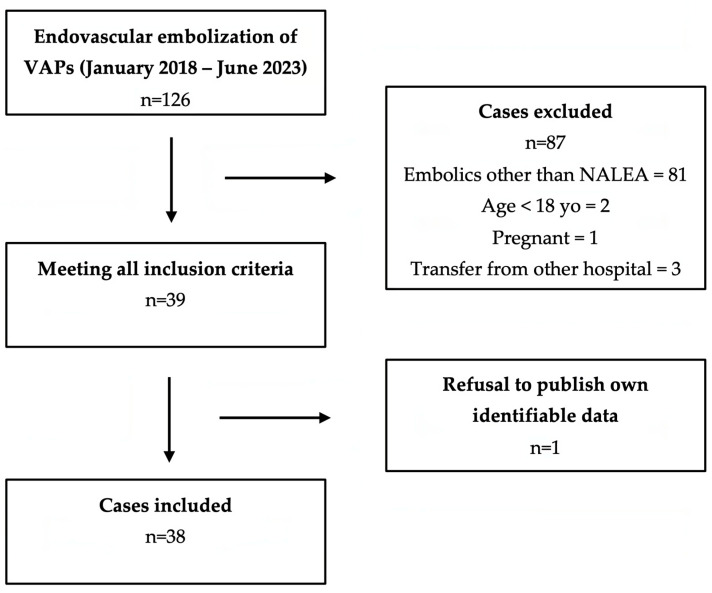
Background and Objectives: Treatment of visceral artery pseudoaneurysms (VAPs) is always indicated regardless of their diameters, as their risk of rupture is significantly higher than that of visceral artery aneurysms. The invasiveness of surgery and its associated complications have led to a shift in favor of radiological interventions as the initial treatment of choice. However, there are still some unanswered questions on endovascular treatment of VAPs regarding the optimal endovascular technique and the efficacy and safety outcomes. The purpose of this multicenter study was to retrospectively evaluate the effectiveness and safety of endovascular treatment of visceral pseudoaneurysms using Ethylene-Vinyl Alcohol (EVOH) Copolymer-Based Non-Adhesive Liquid Embolic Agents (NALEAs). Materials and Methods: Consecutive patients who underwent endovascular embolization with EVOH-based NALEAs for visceral artery pseudoaneurysms between January 2018 and June 2023 were retrospectively evaluated. Results: 38 embolizations were performed. Technical success was achieved in all patients. The clinical success rate was high (92.1% overall), with no significant differences between ruptured and unruptured VAPs (p = 0.679). Seven patients (18.4%) experienced procedure-related complications, related to one case of non-target embolization, four splenic abscesses due to end-organ infarction, and two femoral pseudoaneurysms. The rates of procedure-related complications, end-organ infarction, and vascular access-site complications did not significantly differ between ruptured and unruptured VAPs (p > 0.05). Conclusions: Both ruptured and unruptured visceral pseudoaneurysms can be effectively and safely treated with NALEA-based endovascular embolization. We suggest considering the use of NALEAs, particularly in specific clinical cases that highlight their advantages, including patients with coagulopathy, fragile vessels, and embolization targets that are located at a considerable distance from the microcatheter tip and are otherwise difficult to reach.
Keywords: Ethylene-Vinyl Alcohol; Onyx; embolic agents; embolization; endovascular treatment; non-adhesive liquid embolic agents; percutaneous; pseudoaneurysm; transcatheter arterial embolization; visceral pseudoaneurysms.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources
