

Efficiency of the Cerebroplacental Ratio in Identifying High-Risk Late-Term Pregnancies
- PMID: 37763790
- PMCID: PMC10535994
- DOI: 10.3390/medicina59091670
Efficiency of the Cerebroplacental Ratio in Identifying High-Risk Late-Term Pregnancies
Abstract
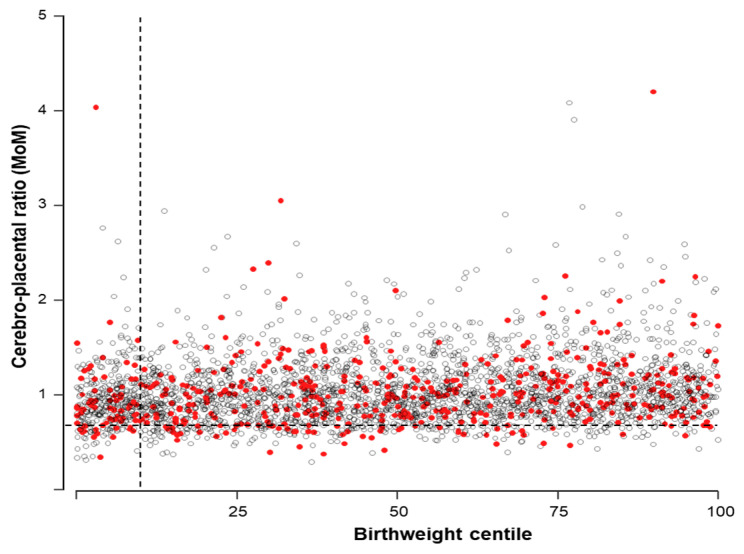
Background and Objectives: Over the last few years, great interest has arisen in the role of the cerebroplacental ratio (CPR) to identify low-risk pregnancies at higher risk of adverse pregnancy outcomes. This study aimed to assess the predictive capacity of the CPR for adverse perinatal outcomes in all uncomplicated singleton pregnancies attending an appointment at 40-42 weeks. Materials and Methods: This is a retrospective cohort study including all consecutive singleton pregnancies undergoing a routine prenatal care appointment after 40 weeks in three maternity units in Spain and the United Kingdom from January 2017 to December 2019. The primary outcome was adverse perinatal outcomes defined as stillbirth or neonatal death, cesarean section or instrumental delivery due to fetal distress during labor, umbilical arterial cord blood pH < 7.0, umbilical venous cord blood pH < 7.1, Apgar score at 5 min < 7, and admission to the neonatal unit. Logistic mixed models and ROC curve analyses were used to analyze the data. Results: A total of 3143 pregnancies were analyzed, including 537 (17.1%) with an adverse perinatal outcome. Maternal age (odds ratio (OR) 1.03, 95% confidence interval (CI) 1.01 to 1.04), body mass index (OR 1.04, 95% CI 1.03 to 1.06), racial origin (OR 2.80, 95% CI 1.90 to 4.12), parity (OR 0.36, 95% CI 0.29 to 0.45), and labor induction (OR 1.79, 95% CI 1.36 to 2.35) were significant predictors of adverse perinatal outcomes with an area under the ROC curve of 0.743 (95% CI 0.720 to 0.766). The addition of the CPR to the previous model did not improve performance. Additionally, the CPR alone achieved a detection rate of only 11.9% (95% CI 9.3 to 15) when using the 10th centile as the screen-positive cutoff. Conclusions: Our data on late-term unselected pregnancies suggest that the CPR is a poor predictor of adverse perinatal outcomes.
Keywords: adverse perinatal outcome; cesarean section; fetal growth restriction; late-term; middle cerebral artery Doppler; stillbirth; umbilical artery Doppler.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Linder N., Hiersch L., Fridman E., Klinger G., Lubin D., Kouadio F., Melamed N. Post-term pregnancy is an independent risk factor for neonatal morbidity even in low-risk singleton pregnancies. Arch. Dis. Child. Fetal Neonatal Ed. 2017;102:F286–F290. doi: 10.1136/archdischild-2015-308553. - DOI - PubMed
-
- Wennerholm U.B., Saltvedt S., Wessberg A., Alkmark M., Bergh C., Wendel S.B., Fadl H., Jonsson M., Ladfors L., Sengpiel V., et al. Induction of labour at 41 weeks versus expectant management and induction of labour at 42 weeks (SWEdish Post-term Induction Study, SWEPIS): Multicentre, open label, randomised, superiority trial. BMJ. 2019;367:l6131. doi: 10.1136/bmj.l6131. - DOI - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
